At a glance
CDC promotes healthy resettlement by providing guidance to panel physicians who conduct health assessments for U.S.-bound refugees. Panel physicians perform medical examinations to identify refugees with significant medical conditions, assess and document their medical needs, and provide pre- and post-travel recommendations to ensure important health needs are met during travel to and immediately after arrival in the United States. Please note that the "Pre-embarkation (Fitness-to-travel) Check" and "Guidance for Overseas Medical Examinations for Refugees with Significant Medical Conditions" sections of this guidance apply only to situations in which IOM or another coordinating agency is organizing travel for refugees.
Attention
This is a companion page to: Supplemental Guidance for Performing the Overseas Medical Examination of Refugees.
Refugees with significant medical conditions
While conducting health assessments for U.S.-bound refugees, panel physicians should identify refugees who have significant medical conditions (SMC) and assess their health-related resettlement needs. The panel physician should use the Significant Medical Conditions (SMC) form to document such health needs. This important documentation helps ensure that the refugee arrives in the United States with an adequate supply of needed medications and medical equipment; is connected to early follow-up care; and is placed in appropriate housing and/or locations if special medical accommodations are needed.
Once the refugee has arrived in the U.S., resettlement support staff -some of whom are non-medical-will refer to the SMC form to arrange follow up services for the refugee. Therefore, panel physicians should document as clearly and completely as possible when completing SMC forms.
The following is a list of SMCs which may prompt additional assistance and coordination during a refugee's resettlement process:
- Pregnancy
- Significant mental illness or developmental delay
- Severe acute malnutrition
- Life-threatening health condition requiring expedited resettlement
- Major travel assistance needs (e.g., medical escort, oxygen, indwelling catheter, nasogastric tube)
- Significant mobility issues requiring wheelchair, stretcher, or special accommodations (including special housing accommodations after arrival)
- Medical issues requiring urgent follow-up within one week after arrival
- Medical issues requiring extensive surgery or treatment (e.g., renal dialysis, complex congenital cardiac conditions)
- Special schooling or employment needs
The following sections outline the process of identification, pre-travel referral and management, and documentation of travel and post-arrival medical needs for refugees with SMCs.
IMPORTANT
Documenting significant medical conditions: The SMC form
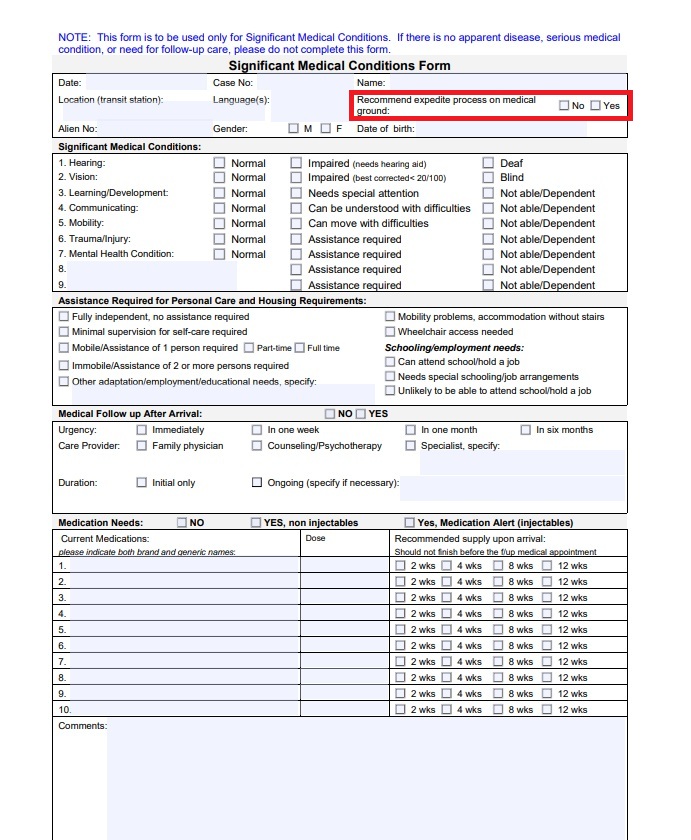
At the conclusion of the health assessment (HA), panel physicians should use the SMC form to document resettlement medical needs of refugees with complex medical conditions. The form contains eight sections:
- Personal and demographic section
- Overall review of SMCs
- Personal care assistance and housing requirements
- Medical follow-up after arrival
- Medication needs
- Medical requirements upon arrival at final destination
- Travel requirements
- Additional comments section
How to complete the significant medical conditions checklist
The first section of the form is meant to gather personal and demographic information about the refugee.
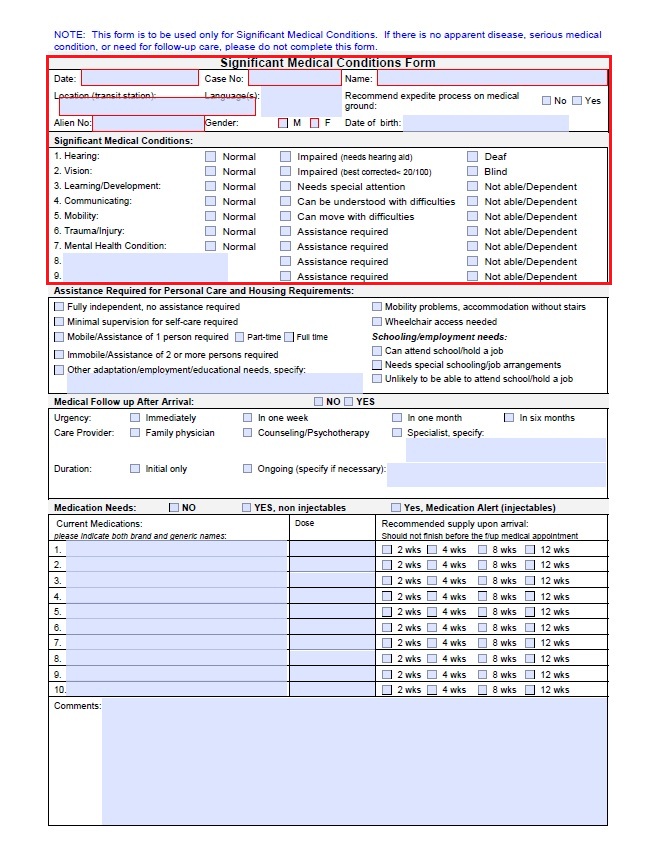
The second section contains a checklist of significant medical conditions to help the panel physician describe how the condition impacts the refugee. These include:
- Hearing: Explain (to the extent possible) in the comments section at the bottom of the SMC form what the person can and cannot hear and how this condition affects their ability to study, work, or perform daily activities. Also indicate current adaptations, such as use of a hearing aid, sign language, or lip reading. An SMC form is not required for medium hearing loss that does not affect schooling, employment, or activities of daily living (ADL).
- Vision: Provide details on the actual disability. Blindness is defined as visual acuity of 20/200 (6/60) or worse in the better eye while the person is wearing corrective lenses. Do not fill out an SMC form for simple refractive errors.
- Learning/Development: Include known or observed developmental delays. Describe any known or observed learning limitations that may affect schooling or work.
- Communication: Detail any communication impairments and adaptations (e.g., speaks single words only or uses sign language) and specify whether the impairment is caused by a particular physical disability/condition, a developmental condition, or a mental health condition.
- Mobility: Determine to the extent possible potential transportation and accommodation needs—including whether wheelchair-accessible housing and/or ADL assistance are needed. Describe each mobility limitation and the underlying cause, ability for self-care, and medical and mobility devices used (e.g., wheelchair). Please indicate if such persons have their own mobility aids or whether such aids should be provided by the resettlement agency (RA) upon arrival, including mobility arrangements needed for children (e.g., stroller or pediatric wheelchair). Children who are unable to sit upright in a car will also require specialized car seats.
- Trauma/Injury: Indicate the type of trauma/injury and provide details about any extra assistance required.
- Mental Health Condition: Whenever possible, indicate post-arrival medical follow-up, assistance, and psychosocial support needs, including any need for a caregiver.
- Other Conditions: Use clinical judgement to determine what additional conditions might represent SMCs and document them in rows eight and nine on the form. For example, the panel physician does not need to document mild to moderate and well-controlled chronic conditions (e.g., hypertension, chronic obstructive pulmonary disease [COPD], diabetes) as these should already be documented on the immigration medical form. But these same conditions, when poorly controlled or severe, must be included on the SMC form to ensure earlier medical follow-up upon arrival.
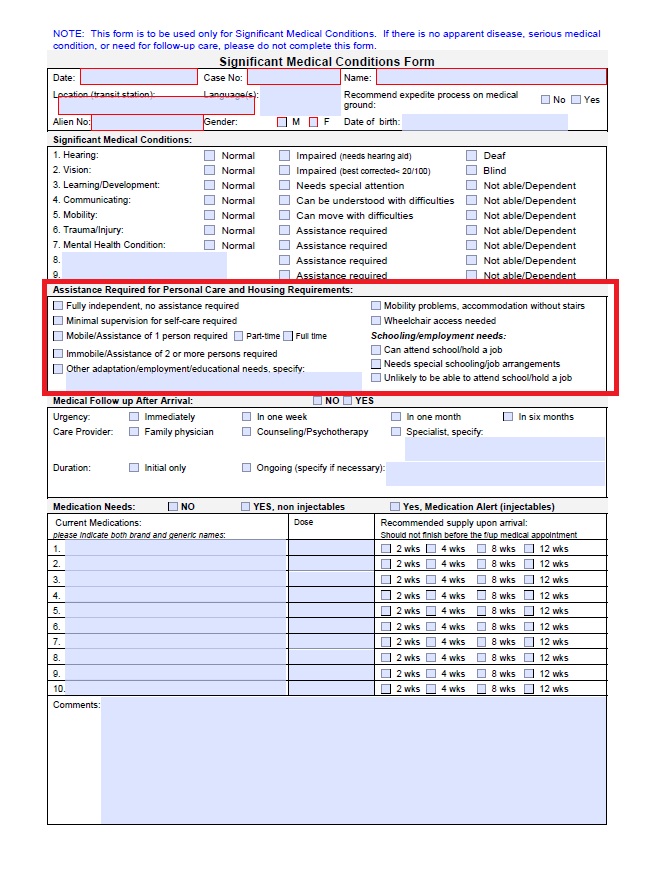
How to document personal care and housing needs
In the third section of the SMC form, the panel physician should document any adaptations needed for personal care, mobility, housing, schooling, or employment.
In addition to the SMC form, there is also an activities of daily living (ADL) form that panel physicians can use to document such needs in greater detail. The panel physician should include the following elements on the ADL form:
- Whether the refugee is capable of independently performing the self-care task or whether they require support, and if so the degree of impairment/functional burden.
- If the refugee needs a caregiver, specify whether one already exists as part of the household or whether one will need to be hired.
Some refugees with SMCs may have specific housing placement and/or community support needs (e.g., schooling, employment, apartment needing to be on the first floor due to wheelchair/mobility issues, etc.) after arrival. The panel physician should indicate these details in the remarks section of the SMC form as clearly as possible. More complex needs should be described in greater detail using the ADL form in addition to the SMC form.
After the HA, panel physicians should complete the form and share it with the resettlement support center (RSC) or the assigned International Organization for Migration (IOM) focal point.
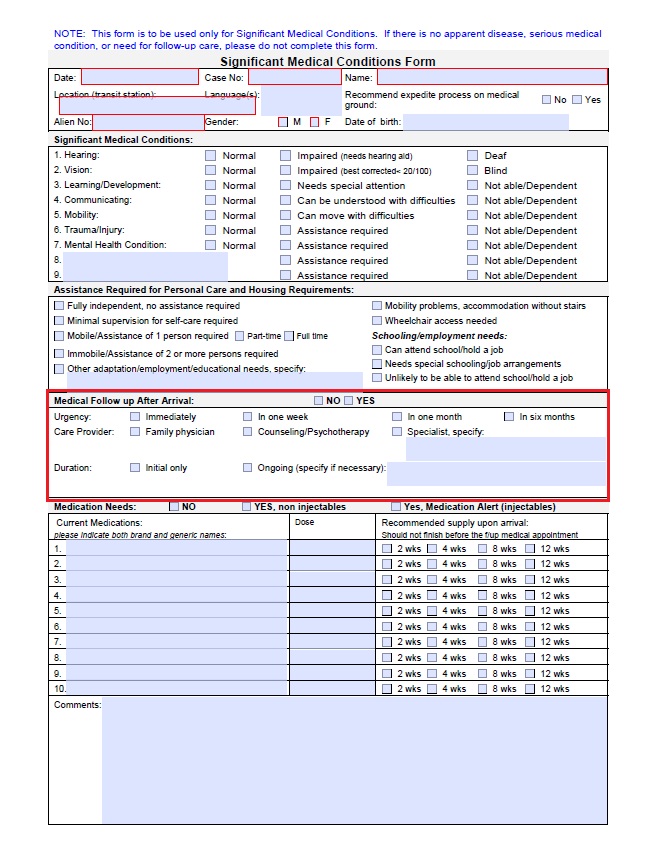
How to document post-arrival medical follow up needs
In this section of the SMC form, panel physicians should document the refugee's medical follow-up needs. Be sure to include how soon after arrival the refugee will need a medical appointment. Refer to the SMC quick reference tables which include suggested post-arrival follow up time frames for different SMCs.
.
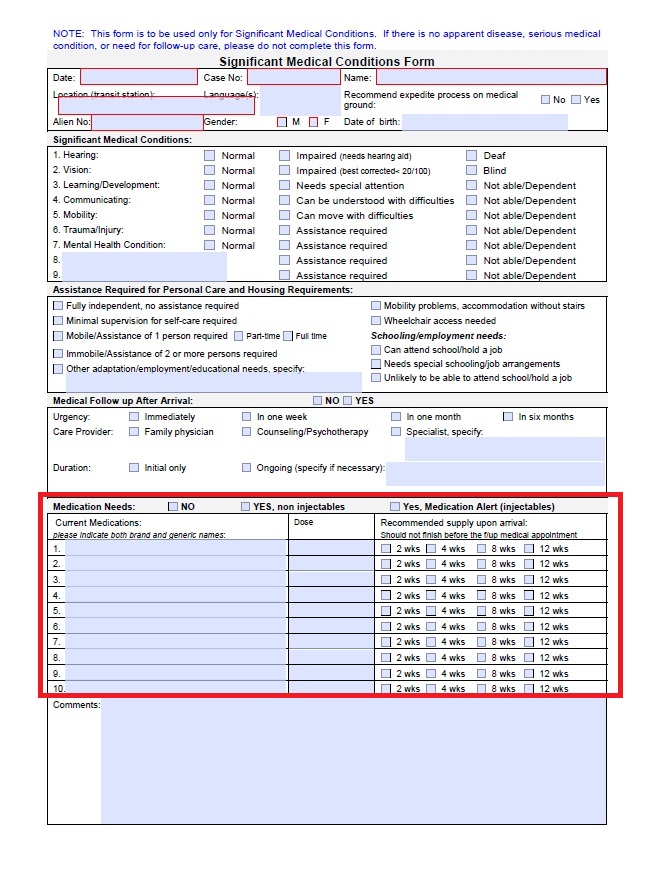
How to document medication needs
In this section of the SMC form, the panel physician should list any medications that the refugee is taking, including dose and frequency. Document the existing medication supply quantity (e.g., "traveling with 12 weeks of medication") so that the RA can plan for medication refills. After arrival in the United States, the refugee must attend a medical appointment to obtain prescription refills.
How to document travel needs
Air travel can worsen some health conditions due to a combination of stress, high altitudes, long flight times, and airplane cabin environment (low humidity, reduced oxygen partial pressure). Therefore, some refugees with SMCs will need special medical arrangements for travel such as oxygen or a medical escort. An example would be a child with a cyanotic cardiac defect.
In these cases:
- Request medical arrangements as needed so that the RSC and IOM can facilitate these arrangements. In cases like the child described above, the specialist following the refugee may have to be consulted to provide specific air travel recommendations.
- Defer travel if a refugee presents with one of the conditions under the "Travel Deferrals" section on this page. Do not permit the refugee to travel until you have evaluated and stabilized the condition and made the needed medical arrangements.
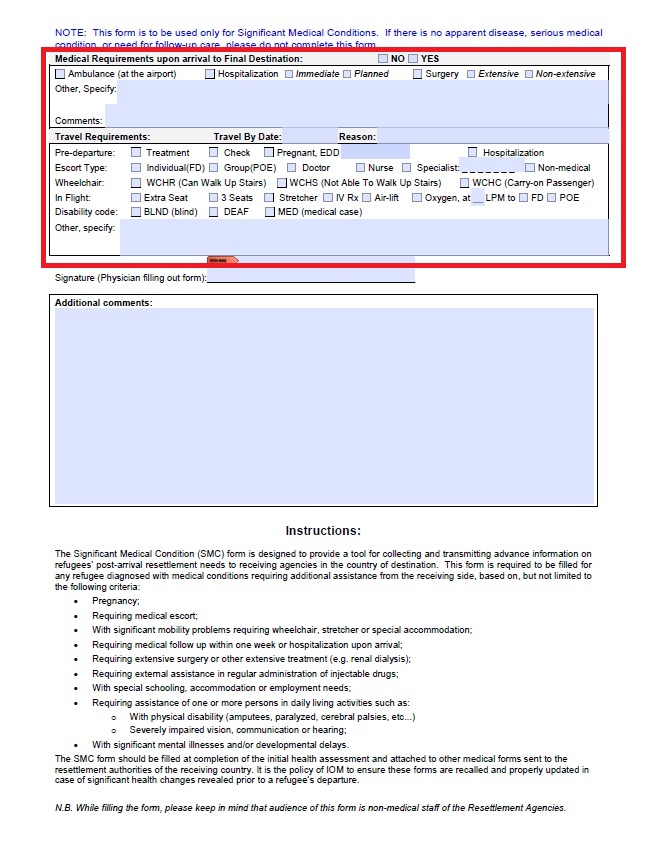
* EDD – estimated delivery date; IV Rx = intravenous therapy; LPM-liters per minute; FD–final destination; Individual FD—1:1 escort accompanying to the final destination; POE–port of entry only; Group POE—group escort accompanying a group of refugees to the port of entry; WCHR—wheelchair, but can walk upstairs and to seat; WCHS—wheelchair, can walk to seat but not upstairs; WCHC—wheelchair, needs to use chair to and from seat
Escort types
A refugee may need a specific type of travel escort depending on their age, medical condition, or disability.
Medical escorts
When IOM is coordinating refugee travel, medical escorts may be assigned to refugees who cannot travel unaccompanied because of their potential need for medical assistance. In general, a person who meets any of the criteria below will need a medical escort. Whether the medical escort is a doctor or nurse will depend on the severity of the condition and the evaluating physician's opinion. Panel physicians should notify IOM (or agency coordinating refugee travel) if a refugee might need a travel escort based on their clinical status. In most cases where a medical escort is needed, the panel physician should check the "Individual FD" box indicating that a 1:1 escort is needed all the way to the final destination. Any other escort categories (e.g., "Group POE" when a group escort is needed) are uncommon and will be arranged directly by IOM. Some examples of refugee travelers needing medical escorts are:
- Refugees with significant medical conditions likely to require treatment during travel.
- Refugees whose condition presents a meaningful risk of clinical deterioration during travel but is not severe enough to prevent travel as described by the International Air Transport Association (IATA) medical guidelines.
- Refugees who require medical devices during travel, including supplemental oxygen, intravenous catheters, indwelling urinary catheters, or nasogastric tubes.
- Refugees with a recent history of medical events such as hospitalization, trauma, surgery, or seizures. Such persons should not travel within the minimum time post-event described in the IATA guidance.
- Refugees with behavioral, cognitive, or intellectual impairments who require supervision or assistance in their daily living activities.
- Refugees with stabilized significant psychiatric illnesses requiring an appropriately trained medical escort.
- Refugees who are frail and/or elderly or children with complex SMC needs who do not have adequate family support.
Operational escorts (non-medical)
This type of escort should be assigned to other categories of refugee travelers, such as:
- Refugees who are healthy unaccompanied minors.
- Refugees who require assistance with mobility but are otherwise clinically well.
- Refugees who have physical impairments, such as visual impairments that require assistance with travel but are otherwise clinically well.
Wheelchair: mobility arrangements
Travel arrangements for refugees with limited mobility may include:
- Access to a wheelchair
- Three-seat seating on the airplane
- Stretcher
In flight: supplemental oxygen
Clearly describe the travel oxygen requirements on the SMC form, including whether the refugee will need oxygen in-flight and on the ground. Include administration instructions (e.g., intermittent or continuous) and how many liters per minute (lpm) should be delivered. Keep in mind that many airlines accept only portable oxygen concentrators (POC) which provide up to 3 lpm continuously. IOM will have to make special arrangements for any higher in-flight oxygen flow requirements.
Special travel considerations for refugees who are pregnant, on dialysis, or have a life-threatening condition
There are time-sensitive travel factors to consider for refugees who are pregnant, are receiving dialysis, or have a life-threatening health condition.
Pregnancy
- Pregnant refugees with gestational age beyond 34 weeks and 6 days cannot travel by air based on IOM practices.
- For refugees with multiparous or complicated pregnancies, the gestational age travel cutoff is reduced to 32 weeks and 6 days.
- For pregnant refugees in their last trimester, or in situations where gestational age cannot be reliably defined, the pre-departure evaluation should include an ultrasound examination to estimate gestational age.
- Panel physicians should always provide a pregnant refugee with a fitness-to-travel certificate that indicates gestational age and estimated delivery date (EDD).
- IOM will provide the pre-departure medical procedures (PDMP) form directly to the panel site when needed.
- Consider pregnant refugees' specific health needs in the context of the resettlement process and provide counseling with the help of the IOM counseling flip chart.
Dialysis
- Any refugee undergoing regular dialysis requires extensive coordination before departure to ensure safe travel within the travel window. The refugee should have a pre-departure dialysis session less than 24 hours before their international flight. The refugee should have another dialysis session upon arrival at the final destination.
- All dialysis patients will need a medical escort.
- Panel physicians should be very diligent about documenting the refugee's dialysis schedule on the SMC and U.S. Department of State medical forms (DS forms). They should include the most recent nephrologist evaluation summaries and relevant laboratory tests.
Life-threatening conditions
A refugee with a life-threatening condition that cannot be addressed otherwise should be considered for expedited resettlement on medical grounds. When completing the SMC form for these patients, panel physicians should check YES for "Recommend expedite process on medical ground' which they will find in the first section of the form. Panel physicians should then provide a detailed explanation in the "comments" section on the last page of the SMC form.
What to put in the comments sections
Remember that these forms are reviewed by non-medical resettlement agency (RA) staff after the refugee arrives in the United States. Utilize the comments sections wisely, conveying key information as clearly and concisely as possible. DO NOT simply copy and paste all the remarks from the DS form into these sections.
In the first "Comments" section, indicate the degree of disability and any needed adaptations, and in the "Additional" comments section, clearly summarize any key medical updates.
Counseling, referrals, and patient management
Once the health assessment is complete, panel physicians should provide counseling to all refugees with significant medical conditions. This should include basic health education on the diagnosed condition(s) and a review of any recommended follow-up, pre-departure, travel, and post-arrival arrangements. This information is also detailed in the IOM counseling flip chart.
Counseling
During counseling, be sure to:
- Name and explain the medical condition(s), recommended medical referrals, and treatment.
- Stress to the refugee the importance of keeping all medical documents accessible, so that medical personnel can refer to these documents during or after travel
- Discuss expected pre-departure and travel arrangements.
- Stress the importance of arranging 8-to-12-weeks supply of medication before departure. The refugee should pack 2 weeks supply in carry-on bags and the remaining supply in checked luggage.
- Explain the importance of follow up with primary, specialist, and emergency health care (depending on the situation) before and after arrival to the United States.
Referrals
To the extent possible, explore medical services and support programs available to refugees with SMCs in your country and refer them when appropriate. In the absence of available free services, please explore other alternatives to address significant medical conditions potentially affecting travel fitness, and coordinate these with the IOM focal points.
If referral to a specialist is needed to determine travel fitness and needs, panels should coordinate with RSC and IOM counterparts for advance approval of referrals and cost.
IOM review and advisory
IOM regional or country medical officers typically conduct a review of medical records for refugees with significant medical conditions. IOM may request additional health information to assist with specialist referrals. The SMC Tables in Annex 1 detail additional evaluations that may be requested for condition-specific travel arrangements.
For SMC cases meeting any of the following criteria, a regular follow-up and management plan (on-site and/or remote follow-up) and pre-departure evaluation (PDE) should be organized with the help of available health care programs, IOM, and/or the panel site:
- Fitness to travel in doubt because of recent illness, hospitalization, injury, surgery, severe acute malnutrition, or instability of an acute or chronic medical condition
- Special travel arrangements are needed, such as escort, oxygen, stretcher, dialysis, etc.
- Known pregnancy
- Newly diagnosed medical condition requiring ongoing medication/treatment
Medical updates
The panel physician should ask refugees to inform them (or RSC/IOM directly) about any significant changes in their medical conditions and any developments such as hospitalizations, surgeries, changes in medication regimen, etc.
Pre-departure evaluation (PDE)
The panel physician should conduct a pre-departure evaluation for refugees with significant medical conditions within 1 to 3 weeks before their departure. This is especially important for refugees whose fitness to travel must be reconfirmed or for refugees who require special medical or mobility arrangements for travel as described in the counseling, referrals, and patient management section. The PDE includes the following components:
- Medical history review and comprehensive physical examination
- Specialist review when indicated to ensure fitness to travel and to advise about travel medical requirements.
- Oxygen saturation measurement for persons with:
- Cardiac or respiratory SMCs
- Anemia
- Shortness of breath on exam
- Hemoglobin measurement for refugees with certain SMCs that pose a health risk during air travel, including:
- Refugees who are pregnant
- Refugees with moderate to severe acute malnutrition (if not previously measured)
- Refugees with sickle cell anemia or thalassemia
- Refugees with splenomegaly
- Refugees with anemia identified at the initial examination or at the PDE
- Refugees with reduced oxygen saturation (if cause is unknown)
- Blood glucose level for refugees with diabetes
- Other investigations as coordinated with IOM
Annex 1: Guidance for Workup of SMCs
The quick reference tables below will help panel physicians prepare for resettlement of refugees with some of the SMCs which may affect travel and placement needs. Please note that this is not an exhaustive list of conditions and is meant to serve as a helpful reference. Regular follow up should be arranged by the panel physician in coordination with IOM. This may involve in-office, telephone, or specialist follow up depending on the condition, needs, and severity. To the extent possible, panel physicians should refer refugees to existing primary healthcare networks in-country in coordination with IOM. In some situations, IOM coordinates the follow up once the panel site notifies them of the SMC details.
Quick Reference for Overseas Medical Examinations for Refugees with Significant Medical Conditions
A special note about children with SMCs
Flag any children with the following conditions for further referral and/or evaluation (either by a pediatrician or another specialist) before departure. This includes children with:
- A significant medical condition, even if stable.
- Moderate to severe acute malnutrition. For all children, weight, height, and WHZ or BMIZ should be compared to HA, PDE (if applicable), and PEC to ensure no deterioration.
- Developmental delays that affect the way the child moves or their ability to feed (e.g., cerebral palsy, delayed gross motor milestones, difficulty with suck/swallow, or other similar conditions).
Each patient is different. Final workup and referral plans are subject to the panel physician's clinical judgement in close coordination with the IOM medical team, while remaining mindful that refugees with SMCs are at risk of medical deterioration during travel and must be properly evaluated for travel fitness.