At a glance
This CDC report provides vaccination coverage data among adolescents aged 13–17 years living in the U.S.-Affiliated Pacific Islands (USAPI) between 2013 and 2024.

Authors
Ashley Tippins, MPH1; E.M. Boyd, MHCA2; Glodi Mutamba, MD, MPH2; Kelsey C. Coy, MPH2; Jennifer L. Kriss, PhD1
1Immunization Services Division, National Center for Immunization and Respiratory Diseases, CDC; 2Eagle Health Analytics, LLC
Summary
The Advisory Committee on Immunization Practices (ACIP) recommends that adolescents aged 11–12 years receive tetanus, diphtheria, and acellular pertussis vaccine (Tdap); quadrivalent meningococcal conjugate vaccine (MenACWY); and human papillomavirus (HPV) vaccine1. Coverage of vaccines recommended earlier in childhood are also monitored in this age group, to assess community-level protection against vaccine-preventable diseases in a school-age population. All six of the U.S.-Affiliated Pacific Islands (USAPI)A participate in the U.S. domestic immunization program. CDC collaborates with USAPI immunization programs to monitor vaccination coverage for all vaccines included in jurisdictional programs.
This report provides vaccination coverage data derived from jurisdictional immunization information Systems (IISs) among adolescents aged 13–17 years in the USAPI from 2013 to 2024B. Adolescent routine vaccination coverage varied widely by jurisdiction, with Commonwealth of the Northern Mariana Islands consistently reporting the highest coverage across most vaccines (≥95%). From 2013 to 2024, HPV vaccination coverage and series completion generally increased across jurisdictions, though progress plateaued or declined for some jurisdictions from 2021 to 2024. Data in this report can be used to determine where additional efforts are needed to assess reasons for delayed vaccination of adolescents, specific to each jurisdiction.
Methods
Data Sources and Inclusion and Exclusion Criteria
Patient-level data from jurisdictional immunization information systems (IISs) were aggregated at the jurisdiction level for this analysis. Individuals were included in the denominator for the adolescent vaccination coverage assessment if they were 1) aged 13-17 years as of January 1, 2025, 2) had an active patient statusC in the IIS, and 3) had a record of any vaccine in the IIS since 2009D.
Individuals were included in the denominator for annual HPV vaccination analyses if they 1) were girls aged 13–17 years as of January 1 of the assessment year, 2) had an active patient status in the IIS through the end of the assessment year, and 3) had a record of any vaccine in the IIS since 2009.
Estimation of Vaccination Coverage
To assess coverage with vaccines recommended by ACIP at age 11 - 12 years, doses received through December 31, 2024 were included for the tetanus, diphtheria, and acellular pertussis vaccine (Tdap) and the quadrivalent meningococcal conjugate vaccine (MenACWY). Assessment of select vaccines recommended in childhood was also conducted to assess community-level protection against vaccine-preventable diseases in a school-age population, and included measles, mumps, and rubella vaccine (MMR), Hepatitis A vaccine (HepA), Hepatitis B vaccine (HepB), and varicella vaccine; doses received through December 31, 2024 were included.
Estimation of HPV Vaccination Coverage Trends
For human papillomavirus (HPV) vaccine, recommended at age 11 - 12 years, a retrospective point-in-time analysis (i.e., coverage as of a specific date) was used to estimate vaccination coverage as of December 31 of each year from 2013- 2024. All HPV vaccine doses received as of the end of the assessment year were included in coverage estimates. Vaccination coverage indicators included receipt of ≥1 HPV vaccine dose and HPV vaccination series completion statusE. Completion of the HPV vaccination series is defined as receipt of ≥3 HPV vaccine doses, or receipt of 2 doses if the series was initiated at age <15 years, and if ≥5 months minus 4 days have elapsed between receipt of the first and second dose.
HPV vaccination series dropout was measured as the proportion of adolescents who had not completed the HPV vaccination series by the end of the assessment year, among those who received the first dose.
SAS software (version 9.4; SAS Institute) was used to conduct all analyses. This activity was reviewed by CDC, deemed not research, and was conducted consistent with applicable federal law and CDC policyF.
Results
Routine Vaccination Coverage Among Adolescents Aged 13–17 Years, by Vaccine Type
For vaccines routinely given in adolescence, coverage varied substantially by jurisdiction and vaccine. Coverage with ≥1 dose Tdap vaccine ranged from 16.7% in the Republic of the Marshall Islands (RMI) to 98.4% in the Commonwealth of the Northern Mariana Islands (CNMI). Coverage with ≥1 dose MenACWY vaccine was 11.4% in RMI, 94.7% in American Samoa, and 97.9% in CNMI; the vaccine is not part of the routine vaccination program in the Federated States of Micronesia (FSM) or Republic of Palau (Palau) (Table 1).
Coverage with vaccines routinely given in childhood were also assessed. For vaccines routinely given in childhood, coverage with ≥2 doses HepA vaccine was 18.6% in RMI, 95.2% in American Samoa, and 96.9% in CNMI; the vaccine is not part of the routine vaccination program in FSM or Palau. Coverage with ≥2 doses MMR vaccine ranged from 85.4% in Palau to 99.4% in CNMI. Coverage with ≥3 doses HepB vaccine ranged from 86.6% in FSM to 99.5% in CNMI. Coverage with ≥2 doses varicella vaccine was 88.4% in American Samoa and 94.2% in CNMI; the vaccine is not part of the routine vaccination program in FSM, Palau, or RMI.
Trends in HPV Vaccination Among Adolescent Females Aged 13–17 Years, 2013–2024
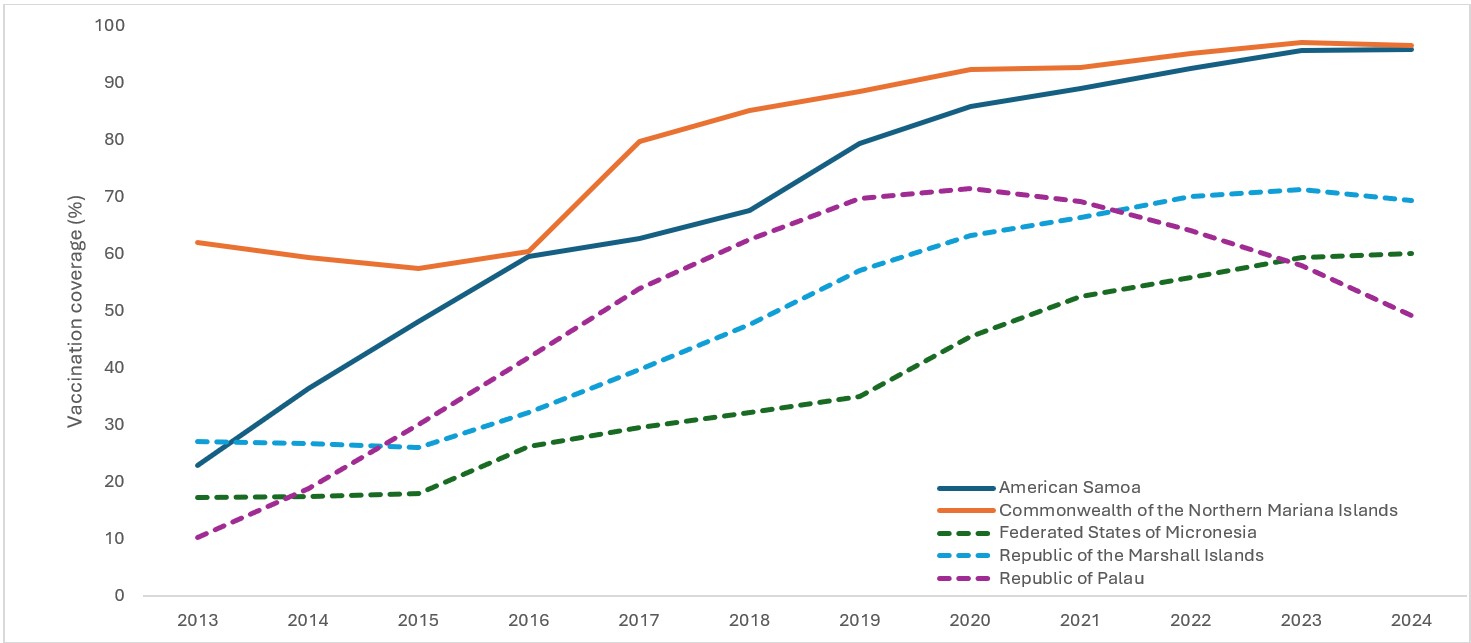
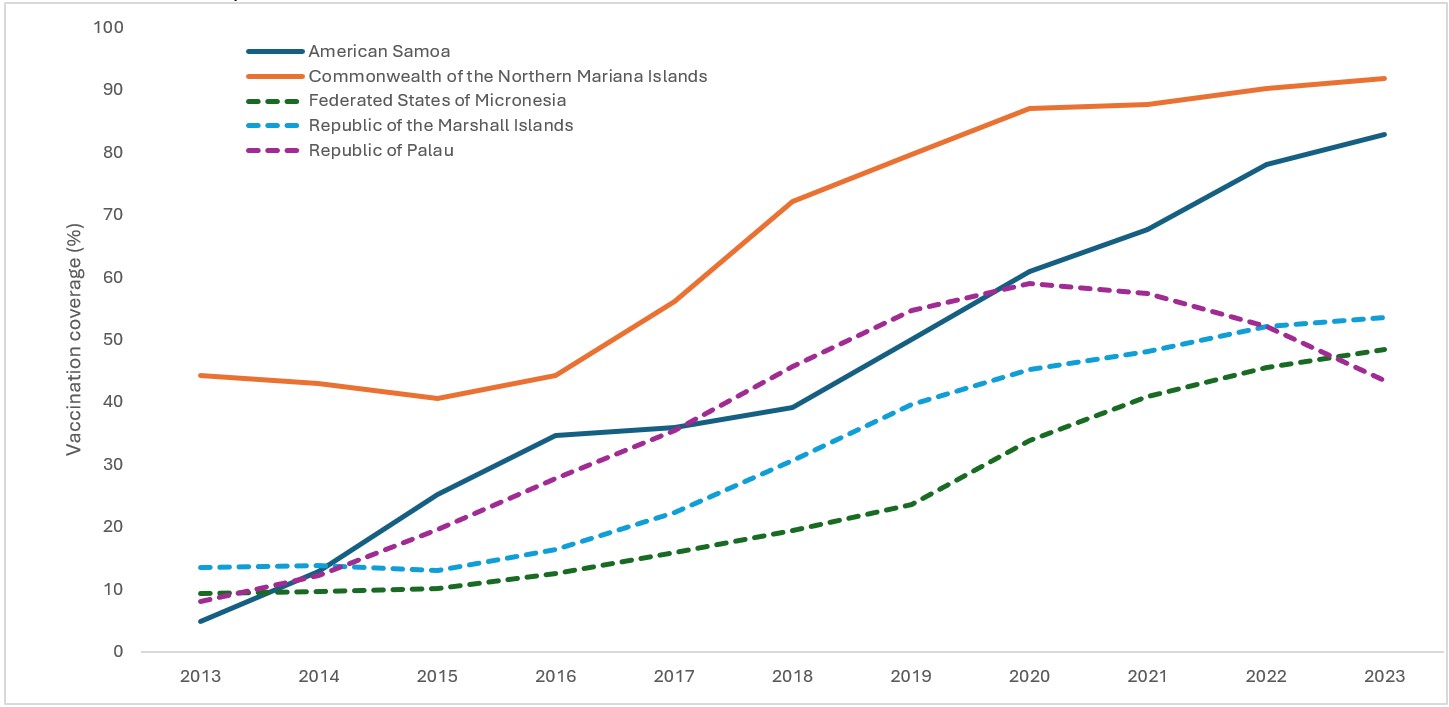
From 2013 to 2024, there was an increase in coverage with ≥1 HPV vaccine dose from 34.6 (CNMI) to 73.0 (American Samoa) percentage points across jurisdictions (Figure 1) and an increase in HPV vaccination series completion coverage from 15.3 (Palau) to 80.0 (American Samoa) percentage points (Figure 2). The percentage of adolescent girls who had received ≥1 HPV vaccine dose and who completed the vaccination series increased each year from 2015 to 2023 in all jurisdictions except Palau. In 2024, coverage decreased 0.5 percentage points in CNMI and 2.0 percentage points in RMI. In Palau, ≥1-dose coverage and HPV vaccination series completion coverage peaked in 2020 at 71.6% and 59.0%, respectively, and have since decreased to 49.2% and 23.4%, respectively, in 2024 (Table 2). Among jurisdictions with continuing increases, year to year changes in coverage has declined, but if coverage in American Samoa and CNMI continues to increase by at least 1 percentage point annually, both jurisdictions will meet the World Health Organization (WHO) 2030 ≥90% HPV vaccination series completion coverage goal.
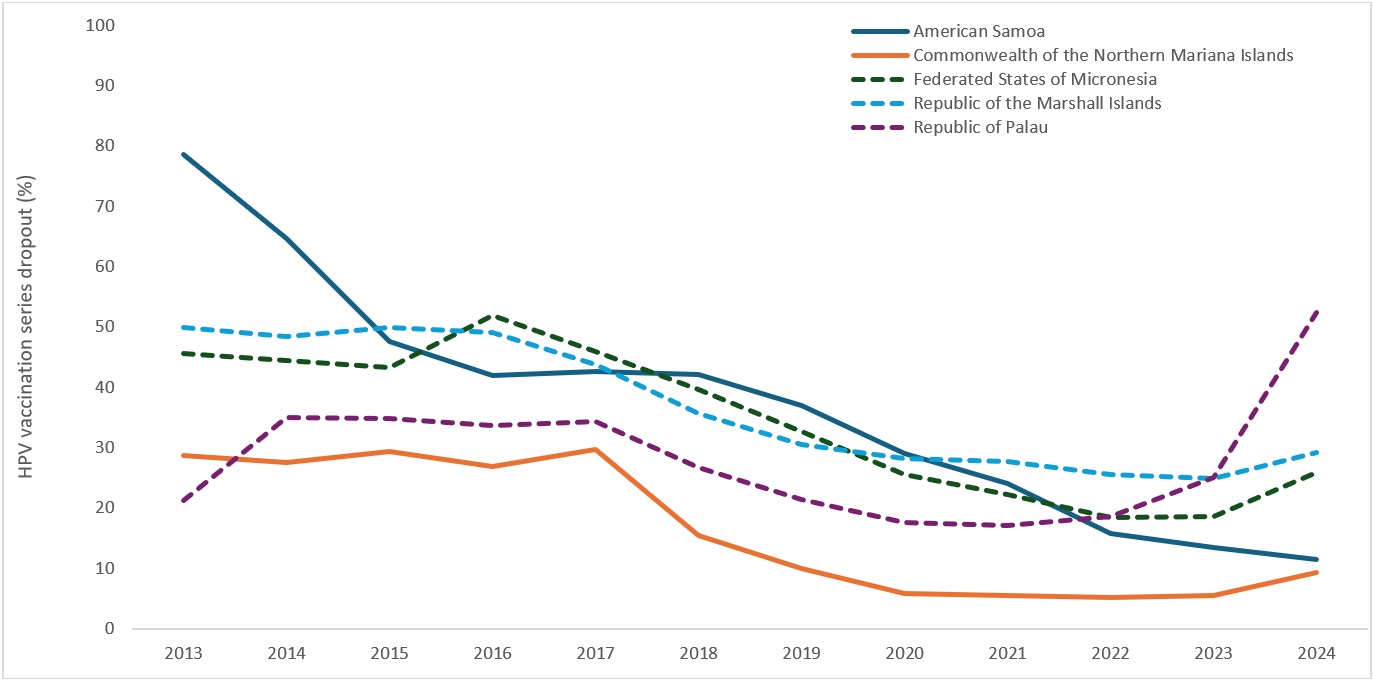
HPV vaccination series dropout varied across jurisdictions and years; from 2013 to 2023, dropout decreased in all jurisdictions except in Palau, where it increased from a low of 17.2% in 2021 to a high of 25.2% in 2023. In 2024, drop-out increased compared to 2023 in all jurisdictions except American Samoa (Figure 3). Dropout was lowest in CNMI, where only 9.4% of adolescent girls aged 13-17 years who initiated the HPV vaccination series had not completed it in 2024 (Table 2).
Discussion
This report provides an analysis of adolescent vaccination coverage across the USAPI, highlighting both significant achievements and persistent challenges. The findings demonstrate that while routine adolescent vaccine coverage is generally high in the U.S. territories, considerable variation exists across the freely associated USAPI jurisdictions.
A notable success story is the substantial increase in HPV vaccination coverage and series completion over the past decade across the USAPI. This progress is particularly encouraging as the HPV vaccine prevents 92% of HPV-attributable cancers2. Among the U.S. territories, American Samoa and the Northern Mariana Islands have achieved high coverage, largely attributable to robust implementation strategies, including a combination of school-located vaccination and providing additional access to the vaccine in public health clinics. Both jurisdictions receive vaccination program funding and vaccine supply through the Section 317 Immunization Program and the U.S. Vaccines for Children (VFC) program.
The three freely associated jurisdictions are not eligible to receive VFC funding and thus have more constrained vaccine supply and funding for program operations; therefore, these jurisdictions have not consistently been able to offer HPV vaccine in locations outside the school setting and have also not been able to implement other routinely recommended vaccines, such as MenACWY. This structural difference translates into lower vaccination coverage for routine adolescent vaccines, and a more challenging trajectory to reach coverage goals for HPV vaccine series completion. These findings reinforce the importance of sustained, well-resourced immunization programming to achieve high vaccination coverage.
Further, the plateauing or decline in HPV vaccination coverage observed in some jurisdictions from 2021 to 2024, particularly the substantial decrease in Palau, signals a need for tailored intervention strategies to address vaccine access and uptake barriers. The increasing HPV vaccination series dropout rates in some jurisdictions further highlight the need for improved follow-up and completion strategies.
To address areas of declining or lagging coverage, immunization programs in the USAPI could conduct in-depth assessments to understand jurisdiction-specific barriers to vaccination, including funding barriers, logistical challenges, cultural beliefs, and healthcare provider practices. Equitable vaccine supply and programmatic support has the potential to close the coverage gap and ensure all USAPI adolescents receive recommended vaccinations. The success of school-located vaccination programs highlights the effectiveness of expanding vaccination opportunities. Exploring and implementing similar models, including leveraging clinics, pharmacies, mobile outreach, and community-located health events, can expand vaccine access. Continued education and empowerment of healthcare providers to recommend all routine adolescent vaccines, including HPV, is also essential; emphasizing the cancer-preventative benefits of the HPV vaccine can enhance parental acceptance3. Further, the data presented in this report serve as a useful tool for identifying areas requiring additional effort. Jurisdictions should continue to regularly review their IIS data to pinpoint specific age groups or communities with low coverage and design targeted outreach strategies.
Limitations
The findings in this report are subject to at least three limitations. First, accuracy of coverage estimates in this assessment depend upon completeness and accuracy of jurisdictional IIS data. Working with the jurisdictions, CDC has found high levels of completeness and accuracy (i.e., consistency in recorded dose dates and product types between paper and IIS records) across the five USAPI IISs included in this assessment through evaluations conducted since 2016; however, IIS data completeness before 2016 has not been evaluated. Second, the active patient population size could be inflated in IISs compared with census estimates because of difficulties tracking out-migration and deaths, which can lead to an underestimation of vaccination coverage. However, recent census data were not available for denominator estimation for all jurisdictions included in this assessment. For this reason, exclusion criteria consistent with the Modeling of Immunization Registry Operations Work Group managing active patient status guidance were applied to retrospectively classify likely active patient status to patients in the IIS for each assessment year4. Finally, vaccination coverage for Guam is assessed via the National Immunization Survey and was not included in this analysis. Differences in vaccination coverage estimation methods might mean that results are not directly comparable with IIS-based estimates for the other USAPI presented in this report.
Acknowledgments
Vince Aguon, Peter Judicpa, Michelle Ruslavage, Alex Turner, CDC; Carter Apaisam, Midion Neth, Jr., Federated States of Micronesia Department of Health and Social Affairs; Merlyn Basilius, Landon Decherong, Palau Ministry of Health and Human Services; Yolanda Masunu, Silimusa Masui, American Samoa Department of Health; Shaun Kileleman, Heather Pangelinan, Emman Parian, Cyji Tenorio, Commonwealth Healthcare Corporation; Edlen Anzures, Noatia Siofilisi, Marshall Islands Ministry of Health.
Tables and Figures
Table 1. Estimated vaccination coverage with selected vaccines and doses among adolescents aged 13–17 years* — U.S.-Affiliated Pacific Islands, 2024
| Tdap ≥1 dose† |
MenACWY§ ≥1 dose |
MMR ≥2 doses |
Hepatitis A vaccine ≥2 doses¶ |
Hepatitis B vaccine ≥3 doses |
Varicella ≥2 doses |
|
|---|---|---|---|---|---|---|
| Percent (%) | ||||||
| American Samoa | 95.5 | 94.7 | 98.0 | 95.2 | 96.9 | 88.4 |
| Commonwealth of the Northern Mariana Islands | 98.4 | 97.9 | 99.4 | 96.9 | 99.5 | 94.2 |
| Federated States of Micronesia | 41.3 | NA | 88.9 | NA | 86.6 | NA |
| Republic of the Marshall Islands | 16.7 | 11.4 | 93.6 | 18.6 | 93.4 | NA |
| Republic of Palau | 28.2 | NA | 85.4 | NA | 90.6 | NA |
Abbreviations: Tdap = tetanus, diphtheria, and acellular pertussis vaccine; MenACWY = quadrivalent meningococcal conjugate vaccine; MMR = measles, mumps, and rubella vaccine; NA = Not applicable.
*Age as of January 1, 2025 and vaccination status as of December 31, 2024.
†Includes percentages receiving Tdap vaccine at age ≥10 years.
§Includes percentages receiving MenACWY or an unknown type of meningococcal vaccine.
¶In July 2020, ACIP revised recommendations for Hepatitis A vaccination to include catch-up vaccination for persons aged 2–18 years who have not previously received Hepatitis A vaccine at any age. https://pubmed.ncbi.nlm.nih.gov/32614811/
Table 2. Human papillomavirus vaccination coverage among female adolescents aged 13–17 years*, by jurisdiction — U.S.-Affiliated Pacific Islands†, 2013–2024
| Year | Population (No.) | Percentage | ||
|---|---|---|---|---|
| Received ≥1 HPV vaccine dose | HPV vaccination UTD§ | HPV vaccination series dropout¶ | ||
| American Samoa | ||||
| 2013 | 3,785 | 23.0 | 4.9 | 78.7 |
| 2014 | 3,888 | 36.5 | 12.9 | 64.7 |
| 2015 | 3,937 | 48.1 | 25.2 | 47.6 |
| 2016 | 3,608 | 59.6 | 34.6 | 41.9 |
| 2017 | 3,580 | 62.8 | 36.0 | 42.7 |
| 2018 | 3,578 | 67.7 | 39.1 | 42.2 |
| 2019 | 3,492 | 79.4 | 50.0 | 37.0 |
| 2020 | 3,291 | 86.0 | 61.0 | 29.1 |
| 2021 | 3,194 | 89.0 | 67.6 | 24.0 |
| 2022 | 3,027 | 92.6 | 78.0 | 15.8 |
| 2023 | 2,921 | 95.7 | 82.8 | 13.5 |
| 2024 | 2,613 | 96.0 | 84.9 | 11.6 |
| Commonwealth of the Northern Mariana Islands | ||||
| 2013 | 3,142 | 62.1 | 44.2 | 28.8 |
| 2014 | 3,155 | 59.4 | 43.0 | 27.6 |
| 2015 | 3,053 | 57.5 | 40.6 | 29.4 |
| 2016 | 2,904 | 60.5 | 44.2 | 26.9 |
| 2017 | 2,733 | 79.8 | 56.1 | 29.7 |
| 2018 | 2,673 | 85.3 | 72.1 | 15.5 |
| 2019 | 2,591 | 88.5 | 79.7 | 9.9 |
| 2020 | 2,476 | 92.4 | 87.0 | 5.8 |
| 2021 | 2,511 | 92.7 | 87.6 | 5.5 |
| 2022 | 2,314 | 95.2 | 90.2 | 5.3 |
| 2023 | 2,289 | 97.2 | 91.8 | 5.6 |
| 2024 | 2,226 | 96.7 | 87.6 | 9.4 |
| Federated States of Micronesia | ||||
| 2013 | 6,807 | 17.3 | 9.4 | 45.7 |
| 2014 | 6,914 | 17.5 | 9.7 | 44.6 |
| 2015 | 6,854 | 18.0 | 10.2 | 43.3 |
| 2016 | 6,853 | 26.2 | 12.6 | 51.9 |
| 2017 | 6,769 | 29.6 | 16.0 | 45.9 |
| 2018 | 6,800 | 32.3 | 19.5 | 39.6 |
| 2019 | 6,789 | 35.1 | 23.6 | 32.8 |
| 2020 | 5,956 | 45.6 | 33.9 | 25.7 |
| 2021 | 5,766 | 52.6 | 40.9 | 22.2 |
| 2022 | 5,539 | 55.9 | 45.6 | 18.4 |
| 2023 | 5,507 | 59.5 | 48.4 | 18.7 |
| 2024 | 5,416 | 60.1 | 44.5 | 26.0 |
| Republic of the Marshall Islands | ||||
| 2013 | 3,358 | 27.2 | 13.6 | 50.0 |
| 2014 | 3,400 | 26.8 | 13.8 | 48.5 |
| 2015 | 3,373 | 26.0 | 13.0 | 50.0 |
| 2016 | 3,368 | 32.2 | 16.4 | 49.1 |
| 2017 | 3,402 | 39.7 | 22.3 | 43.8 |
| 2018 | 3,475 | 47.7 | 30.7 | 35.6 |
| 2019 | 3,528 | 57.2 | 39.7 | 30.6 |
| 2020 | 3,518 | 63.2 | 45.3 | 28.3 |
| 2021 | 3,476 | 66.5 | 48.1 | 27.7 |
| 2022 | 3,231 | 70.2 | 52.2 | 25.6 |
| 2023 | 2,981 | 71.4 | 53.6 | 24.9 |
| 2024 | 2,750 | 69.4 | 49.1 | 29.3 |
| Republic of Palau | ||||
| 2013 | 893 | 10.3 | 8.1 | 21.4 |
| 2014 | 786 | 18.8 | 12.2 | 35.1 |
| 2015 | 721 | 30.1 | 19.6 | 34.9 |
| 2016 | 673 | 41.9 | 27.8 | 33.7 |
| 2017 | 683 | 54.0 | 35.4 | 34.4 |
| 2018 | 650 | 62.6 | 45.8 | 26.8 |
| 2019 | 647 | 69.7 | 54.7 | 21.5 |
| 2020 | 630 | 71.6 | 59.0 | 17.6 |
| 2021 | 639 | 69.3 | 57.4 | 17.2 |
| 2022 | 623 | 64.2 | 52.2 | 18.7 |
| 2023 | 629 | 58.0 | 43.4 | 25.2 |
| 2024 | 598 | 49.2 | 23.4 | 52.4 |
Abbreviations: HPV = Human papillomavirus; UTD = Up to date.
*Vaccination status as of December 31 each year, age as of January 1 the following year.
†Jurisdictions in this report include American Samoa, Commonwealth of the Northern Mariana Islands, Federated States of Micronesia, Republic of the Marshall Islands, and Republic of Palau. Vaccination coverage among adolescents in Guam has been assessed via the National Immunization Survey since 2013; Immunization Information System-based coverage assessment was not conducted for Guam. See https://www.cdc.gov/teenvaxview/interactive/ for adolescent vaccination coverage in Guam.
§In December 2016, the HPV vaccination recommendations changed from a 3-dose series for all to a 2-dose series among children who initiate the vaccine series before age 15 years. An up-to-date measure that determines if the child received either ≥2 or ≥3 HPV vaccine doses, according to recommendations based on age-at-initiation and time intervals between doses, was applied retrospectively for all years during 2013–2023. The HPV vaccination UTD measure includes receipt of ≥3 doses, and receipt of 2 doses when the first HPV vaccine dose was initiated at age <15 years and ≥5 months minus 4 days had elapsed between the first and second doses (https://www.cdc.gov/vaccines/programs/iis/cdsi.html).
¶The percentage of adolescents who started the HPV vaccination series but did not complete it.
Figure 1. Trends in ≥1 dose human papillomavirus vaccination coverage among female adolescents aged 13–17 years*, by jurisdiction† — U.S.-Affiliated Pacific Islands, 2013–2024
Abbreviations: HPV = Human papillomavirus.
*Vaccination status as of December 31 each year, age as of January 1 the following year.
†Jurisdictions in this report include American Samoa, Commonwealth of the Northern Mariana Islands, Federated States of Micronesia, Republic of the Marshall Islands, and Republic of Palau. Vaccination coverage among adolescents in Guam has been assessed via the National Immunization Survey since 2013; Immunization Information System-based coverage assessment was not conducted for Guam. See https://www.cdc.gov/teenvaxview/interactive/ for adolescent vaccination coverage in Guam.
Figure 2. Trends in human papillomavirus up to date* vaccination coverage among female adolescents aged 13–17 years†, by jurisdiction§ — U.S.-Affiliated Pacific Islands, 2013–2024
Abbreviations: HPV = Human papillomavirus.
*In December 2016, the HPV vaccination recommendations changed from a 3-dose series for all to a 2-dose series among children who initiate the vaccine series before age 15 years. An up-to-date measure that determines if the child received either ≥2 or ≥3 HPV vaccine doses, according to recommendations based on age-at-initiation and time intervals between doses, was applied retrospectively for all years during 2013–2023. The HPV vaccination UTD measure includes receipt of ≥3 doses, and receipt of 2 doses when the first HPV vaccine dose was initiated at age <15 years and ≥5 months minus 4 days had elapses between the first and second doses (https://www.cdc.gov/iis/cdsi/).
†Vaccination status as of December 31 each year, age as of January 1 the following year.
§Jurisdictions in this report include American Samoa, Commonwealth of the Northern Mariana Islands, Federated States of Micronesia, Republic of the Marshall Islands, and Republic of Palau. Vaccination coverage among adolescents in Guam has been assessed via the National Immunization Survey since 2013; Immunization Information System-based coverage assessment was not conducted for Guam. See https://www.cdc.gov/teenvaxview/interactive/ for adolescent vaccination coverage in Guam.
Figure 3. Trends in human papillomavirus vaccination series dropout* among female adolescents aged 13–17 years†, by jurisdiction§ — U.S.-Affiliated Pacific Islands, 2013–2024
Abbreviations: HPV = Human papillomavirus.
*The percentage of adolescents who started the HPV vaccination series but did not complete it (i.e., not up to date). In December 2016, the HPV vaccination recommendations changed from a 3-dose series for all to a 2-dose series among children who initiate the vaccine series before age 15 years. An up-to-date measure that determines if the child received either ≥2 or ≥3 HPV vaccine doses, according to recommendations based on age-at-initiation and time intervals between doses, was applied retrospectively for all years during 2013–2023. The HPV vaccination UTD measure includes receipt of ≥3 doses, and receipt of 2 doses when the first HPV vaccine dose was initiated at age <15 years and ≥5 months minus 4 days had elapses between the first and second doses (https://www.cdc.gov/iis/cdsi/).
†Vaccination status as of December 31 each year, age as of January 1 the following year.
§Jurisdictions in this report include American Samoa, Commonwealth of the Northern Mariana Islands, Federated States of Micronesia, Republic of the Marshall Islands, and Republic of Palau. Vaccination coverage among adolescents in Guam has been assessed via the National Immunization Survey since 2013; Immunization Information System-based coverage assessment was not conducted for Guam. See https://www.cdc.gov/teenvaxview/interactive/ for adolescent vaccination coverage in Guam.
- The U.S.-Affiliated Pacific Islands comprise three U.S. territories (American Samoa, Northern Mariana Islands, and Guam) and three freely associated nations under the Compacts of Free Association (Federated States of Micronesia, Republic of the Marshall Islands, and Republic of Palau). All jurisdictions receive Section 317 Immunization Program funding, which is a discretionary program to purchase vaccines and support immunization infrastructure. The U.S. territories also receive Vaccines for Children (VFC) funding; VFC is an entitlement program, created by the Omnibus Budget Reconciliation Act (OBRA), that provides vaccines at no cost to eligible children aged ≤18 years through enrolled health care providers. The VFC program is administered in all U.S. states, the District of Columbia, U.S. territories, and select large U.S. metropolitan cities and counties (in addition to their respective state programs), in accordance with Section 1928 of the Social Security Act.
- Jurisdictions in this report include American Samoa, Northern Mariana Islands, Federated States of Micronesia, Republic of the Marshall Islands, and Republic of Palau. Vaccination coverage among children in Guam has been assessed via the National Immunization Survey since 2013; IIS-based coverage assessment was not conducted for Guam. Information on childhood vaccination coverage in Guam is available at https://www.cdc.gov/childvaxview/about/interactive-reports.html for childhood vaccination coverage in Guam.
- Patient active or inactive status in the IIS establishes a classification of individual patients within a health care organization. Health care providers are responsible for vaccinating patients with an "active" status within their clinic population or geographic catchment area. Patient status is changed to "inactive" when the patient changes providers, moves, or is lost to follow-up, or "deceased" if patient death is confirmed through manual review or system linkage with vital statistics or other health records. https://repository.immregistries.org/files/resources/5835adc2dad8d/mirow_pais_mini-guide.pdf
- Exclusion criteria consistent with the Modeling of Immunization Registry Operations Work Group managing active patient status guidance was retrospectively applied to mitigate IIS denominator inflation (cf. 4). Patients were excluded from all analyses if they had zero vaccine doses recorded in the IIS or if the last vaccination date recorded in the IIS was before January 1, 2009.
- In 2016, the HPV vaccine recommendations changed from a 3-dose series for all to a 2-dose series among children and adolescents who initiate the vaccination series before age 15 years. Completion of the HPV vaccination series is defined as receipt of ≥3 HPV vaccine doses or receipt of 2 doses if the series is initiated at age <15 years, and ≥5 months minus 4 days have elapsed between the first and second dose. This measure was applied retrospectively for all years 2013–2023. https://www.cdc.gov/vaccines/hcp/imz-schedules/child-adolescent-notes.html#note-hpv
- 45 C.F.R. part 46, 21 C.F.R. part 56; 42 U.S.C. Sect. 241(d); 5 U.S.C. Sect. 552a; 44 U.S.C. Sect. 3501 et seq.
- CDC. "Child and Adolescent Immunization Schedule by Age." Vaccines & Immunizations, 6 June 2025, https://www.cdc.gov/vaccines/hcp/imz-schedules/child-adolescent-age.html
- Senkomago V, Henley SJ, Thomas CC, Mix JM, Markowitz LE, Saraiya M. Human papillomavirus–attributable cancers—United States, 2012–2016. MMWR Morb Mortal Wkly Rep 2019;68:724–8. https://doi.org/10.15585/mmwr.mm6833a3PMID:31437140
- CDC. "Talking with Parents about HPV Vaccination." Human Papillomavirus (HPV), 15 Jul. 2024, https://www.cdc.gov/hpv/hcp/vaccination-considerations/talking-with-parents.html.
- American Immunization Registry Association Modeling of Immunization Registry Operations Work Group. Management of patient active/inactive status in immunization information systems. Atlanta, GA: American Immunization Registry Association; 2015. https://repository.immregistries.org/files/resources/5835adc2dad8d/mirow_pais_full_guide.pdf