At a glance
Overview
CDC expects the upcoming U.S. fall and winter respiratory disease season will likely have a similar combined number of peak hospitalizations due to COVID-19, influenza, and RSV compared to last season. CDC's outlook is based on historical trends, expert opinion, and scenario modeling results.
This outlook serves as a baseline for what could occur during the 2025-2026 season. It is intended to provide decision-makers with information to assist in public health preparedness for respiratory virus illnesses during the 2025-2026 fall and winter respiratory season (defined as October through mid-May). This includes when hospitals might experience the most demand due to COVID-19, influenza, and RSV. We will update this outlook every two months or as warranted during the respiratory season.
To develop this outlook, we consulted a range of CDC and external experts on COVID-19, influenza, RSV, and infectious disease dynamics to assess what may occur during the 2025-2026 season. Our assessments are based on expert elicitation; historical data for COVID-19, influenza, and RSV; and COVID-19 scenario modeling conducted by the Center for Forecasting and Outbreak Analytics (CFA). Similar methods used in the past two respiratory seasons produced outlooks that provided useful ranges and captured the final combined peak hospitalization. As with all long-range outlooks, there is inherent uncertainty, which we describe below. This is a high-level assessment intended to provide information on how the 2025-2026 respiratory season could unfold, and it is not a precise forecast.
We use COVID-19, RSV, and influenza-associated peak hospitalization rates to understand trends in disease-specific and combined burden throughout the respiratory season. While peak hospitalization rate is a key factor for this outlook and contributes substantially to hospital burden, cumulative disease burden will also impact hospital demand throughout the season. It is possible that there will be multiple peaks in the combined hospitalization burden this season.
Combined burden
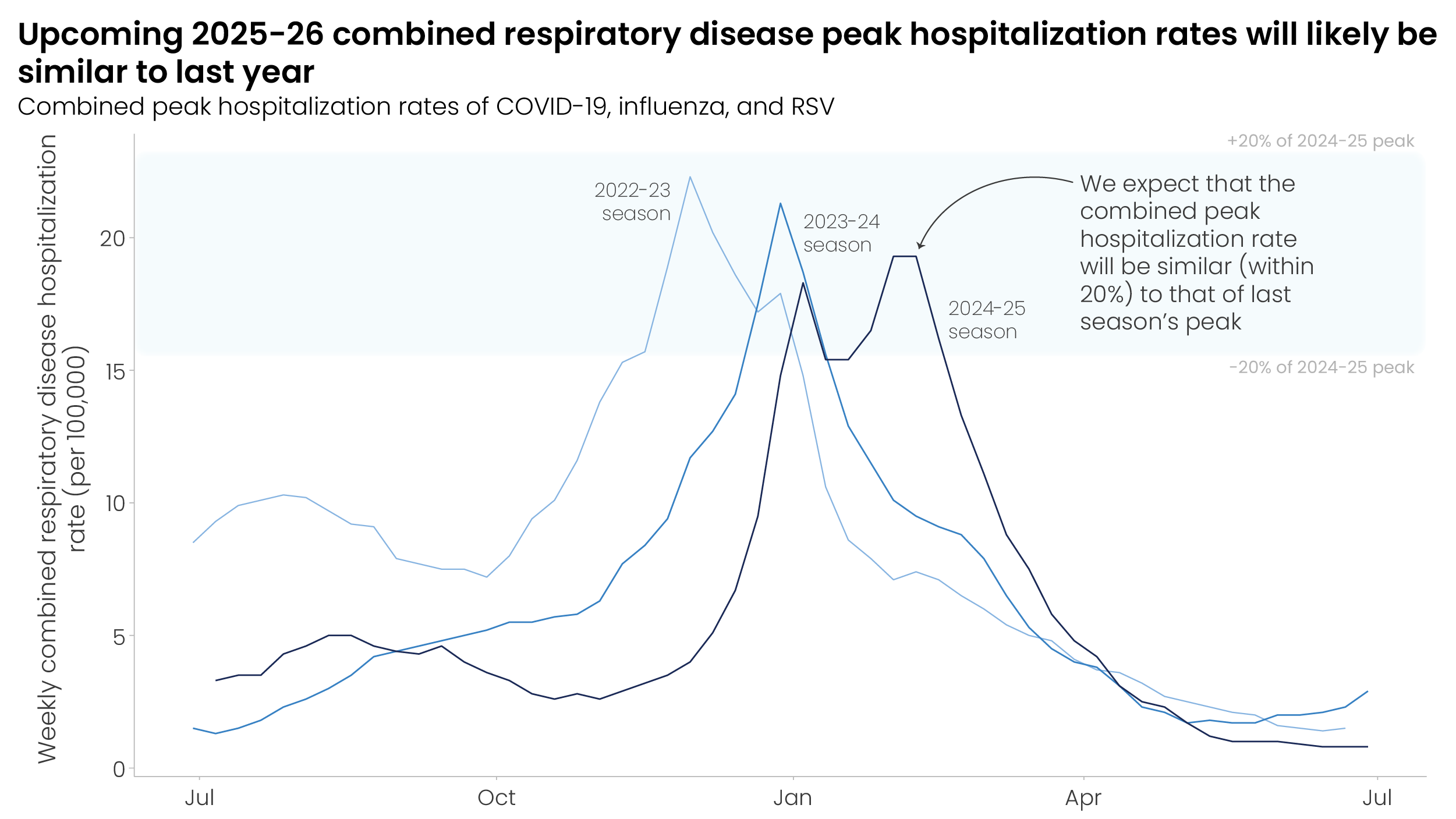
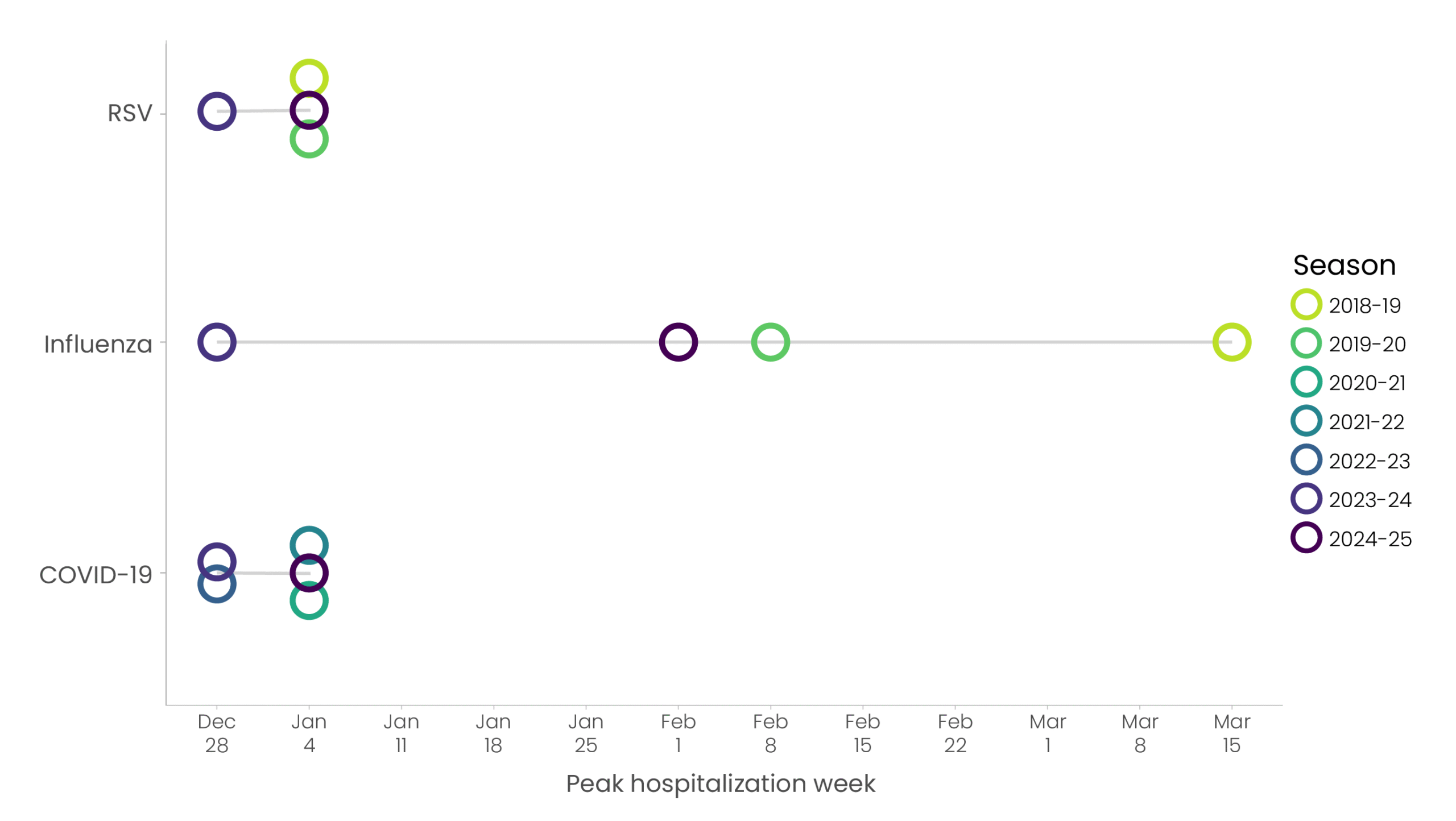
CDC expects that the combined peak hospitalization rate due to COVID-19, influenza, and RSV will be similar (within 20% of the 2024-2025 peak) to that of last season, with low to moderate confidence, based on historical trends, expert opinion, and scenario modeling results. Combined peak hospitalization burden depends on the timing as well as the magnitude of each disease peak during the respiratory season. There is historic variability in both the timing and magnitude of hospital demand for each of the three diseases. Past data show substantial variation in the timing of disease-specific seasonal peaks by region and across seasons (Appendix Figure). However, in the past three years, the magnitude of combined peak hospitalizations has been relatively consistent (Figure 1, RESP-NET). We consulted a range of CDC and external experts on COVID-19, influenza, RSV, and infectious disease dynamics to assess what could occur during the fall and winter respiratory season. In our questionnaire, experts assessed with low to moderate confidence that the peak combined hospitalization rate for the 2025-2026 season will most likely be similar (within 20%) to that of the 2024-2025 season (Figure 1).
In considering what may occur during the 2025-2026 season, we note the following considerations for each disease:
- COVID-19: As of August 19, 2025, COVID-19 summer disease activity is increasing in much of the United States, which may impact the timing and magnitude of COVID-19 activity during the fall and winter respiratory season. Scenario modeling indicates that the peak weekly hospitalization rate due to COVID-19 may be higher than that of the 2024-2025 season, particularly if a variant with moderate immune-escape properties emerges this fall. See more details in the COVID-19 outlook section below.
- Influenza: The 2024-2025 influenza season was classified as a high-severity season and was the primary driver for the combined disease burden last season. The occurrence of consecutive high-severity seasons has not been observed since CDC began systematically assessing the severity of the influenza season during the 2003-2004 season, but remains possible. See more details in the influenza outlook section below.
- RSV: New immunization products became available for those at highest risk of hospitalization due to RSV (infants and older adults) in 2023 and led to an overall reduction in hospitalizations due to RSV last season. See more details in the RSV outlook section below.
While this season's combined peak hospitalization rate is expected to be similar to that of last year, a higher combined peak rate remains possible. This underscores the need to plan and prepare for the possibility of a higher peak, which could be driven by the following factors:
- Emergence of a new SARS-CoV-2 variant with an increased ability to evade the body's prior immunity, or a new variant associated with higher clinical severity
- Predominance of an influenza subtype with more severe outcomes
- Lower vaccine uptake or effectiveness, including:
- Lower than expected uptake of the COVID-19 vaccine, influenza seasonal vaccine, or RSV immunizations
- Lower effectiveness against COVID-19-, influenza-, or RSV-associated hospitalizations than for the 2024-2025 immunizations
It is difficult to predict the magnitude and timing of peak activity for each disease, as well as how disease-specific timing might overlap. Experts agree that some level of overlap in peak hospitalization burden may occur. COVID-19 hospitalizations during the fall and winter typically peak in late December or early January nationally. Influenza seasons typically peak nationally between December and February each year, but timing within this range is less predictable. The RSV national peak tends to occur in late December or early January, but peaks have historically varied by HHS region, with the Southeast U.S. region peaking earlier than North and West U.S. regions.
COVID-19 outlook
CDC expects that the peak weekly hospitalization rate due to COVID-19 for the 2025-2026 season will be similar to or higher than that of the 2024-2025 season, with moderate confidence, based on historical trends, expert opinion, and scenario modeling results. The emergence of a variant with moderate immune-escape properties this fall could contribute to a higher peak weekly COVID-19 hospitalization rate, according to scenario modeling results. Fall and winter COVID-19 hospitalization rates during the 2025-2026 season will depend on several factors, including:
- Summer 2025 activity: The timing and magnitude of COVID-19 activity during the summer may influence the timing and magnitude of COVID-19 activity during the fall and winter respiratory season.
- Emergence of new variants: If a SARS-CoV-2 variant emerges with substantial immune escape, it could lead to higher transmission and hospitalization rates in the fall and winter.
- Vaccination uptake and effectiveness: It is uncertain how vaccination uptake will change this season, compared to past seasons. Lower vaccine uptake or reduced effectiveness may contribute to increased COVID-19 disease activity this fall and winter.
In each of the past three years, COVID-19 waves have occurred in both the summer and winter. The large 2024 summer wave may have contributed to the lower peak hospitalization rate during the 2024-2025 respiratory season, due to higher levels of population immunity. As of August 19, 2025, COVID-19 hospitalization rates are below levels observed during the same period in prior seasons, although COVID-19 hospitalization rates are increasing in much of the United States.
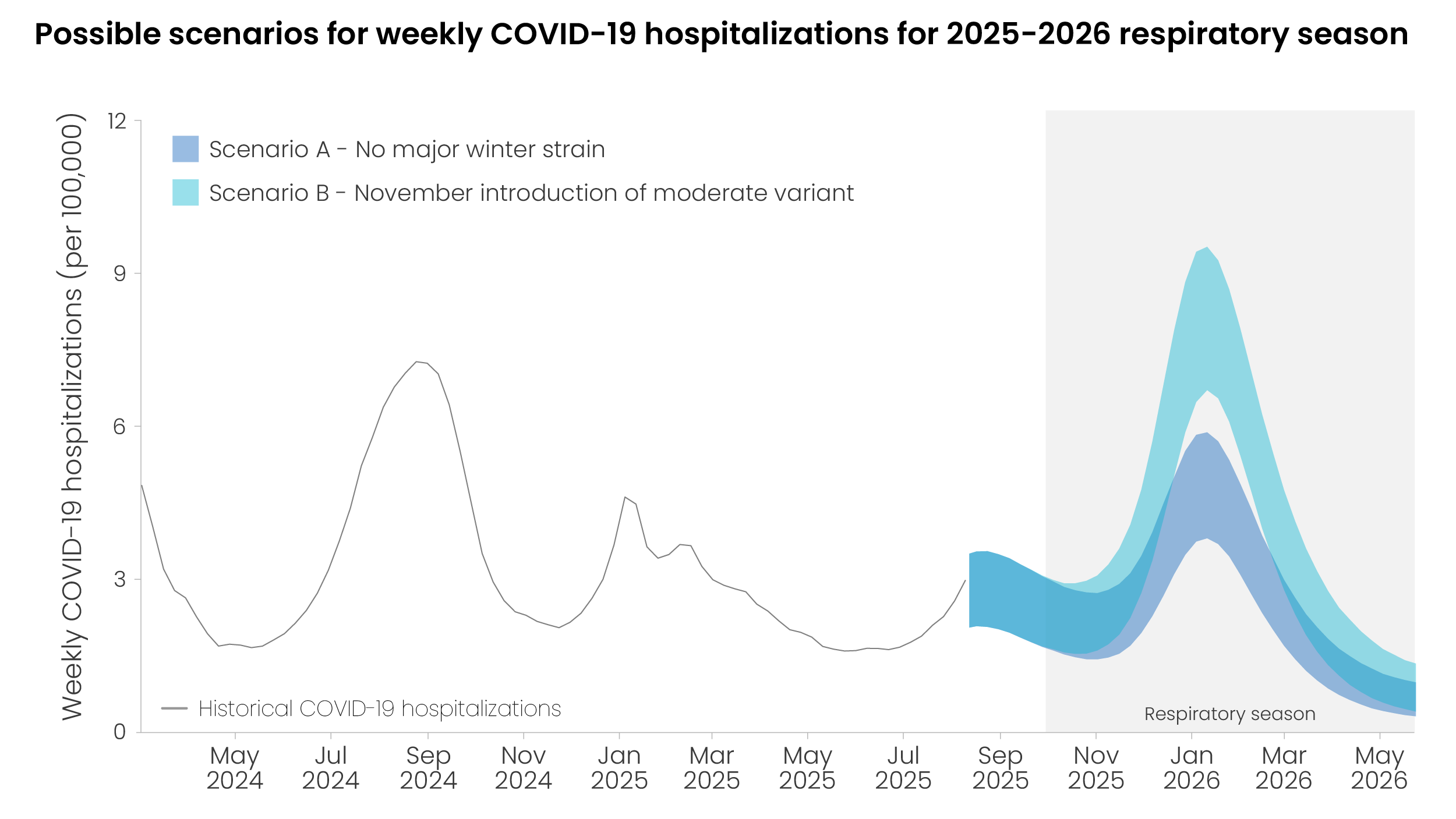
Scenario modeling can be used to assess what could occur during the fall and winter respiratory season. We developed two COVID-19 hospitalization burden scenarios for the 2025-2026 respiratory season to demonstrate the range of possibilities for how the 2025-2026 season could unfold, based on the possible emergence of a variant with moderate immune-escape properties (similar to what was observed from variants that emerged in the United States in the past year) (Figure 2). If a variant with moderate immune-escape properties does not emerge, modeling indicates that the peak weekly COVID-19 hospitalization rate would be between 3.8 and 5.9 hospitalizations per 100,000 (Scenario A). Even without a major winter strain with moderate immune-escape properties, COVID-19 hospitalization rates during the fall and winter of 2025-2026 may be higher than that of last season, due to decreased population immunity following the projected relatively mild summer wave.
If a variant emerges during the fall and winter respiratory season that has moderate immune-escape properties (e.g., is different enough from recently circulating variants), modeling suggests a higher peak weekly COVID-19 hospitalization rate (6.7-9.5 hospitalizations/100,000; Scenario B). Modeling suggests that the national peak hospitalization burden will occur in January in both scenarios, regardless of whether a variant with moderate immune-escape properties emerges.
In this model, we assume that only high-risk groups (defined as those 65 years or older and those with underlying health conditions) will receive the 2025-2026 COVID-19 vaccine, that vaccine uptake within these groups is at the same level as it was during the 2024-2025 season, and that COVID-19 vaccine effectiveness is equal to that of last year. In Scenario A, it is assumed that no variant will emerge that significantly evades the population's immunity. In Scenario B, we assume that a variant with similar properties to the variants that drove the 2024 summer and winter peaks are introduced in NovemberA. See our scenario modeling methods section below for more information.
Recent scenario modeling results from the COVID-19 Scenario Modeling Hub indicate that two periods of increased COVID-19 activity are expected, with a first peak projected in late August 2025 and a second peak projected in January 2026.
Influenza outlook
CDC expects that the severity of the 2025-2026 influenza season based on the peak week of influenza hospitalizations will likely be classified as moderate across all ages, with moderate confidence, based on historical trends and expert opinion. Past seasons have varied widely in the number of illnesses, hospitalizations, and deaths, depending on the subtypes circulating, population immunity to different subtypes, and vaccine effectiveness against circulating subtypes.
The 2024-2025 influenza season was classified as a high-severity season across all ages, making it the first high-severity influenza season since the 2017-2018 season. High-severity seasons are less common than moderate-severity seasons and have not occurred back-to-back since CDC began quantitatively assessing seasonal severity during the 2003-2004 season. However, it remains possible that the influenza season will be of high severity in one or more age groups this season.
Vaccination will play a key role in reducing influenza hospitalization burden this season. Influenza vaccines prevented an estimated 240,000 hospitalizations during the 2024-2025 season, primarily in adults aged 65 years and older. It is uncertain how vaccination uptake and vaccine effectiveness will change this season compared to past seasons.
RSV outlook
CDC expects that the 2025-2026 peak weekly hospitalization rate across all age groups due to RSV will be similar (within 20%) to that of the 2024-2025 season, with moderate confidence, based on historical trends and expert opinion. New RSV immunization products became available for both infants (monoclonal antibodies and maternal vaccination) and adults (vaccination) in 2023. Most experts expect that uptake of these products will continue to increase in the 2025-2026 season, as the public becomes more familiar with their availability and impact.
Vaccination and immunization will continue to play a key role in reducing RSV-associated hospitalization burden this season. During the 2024-2025 season, RSV-associated hospitalization rates among infants aged <8 months in two surveillance networks were lower by 28% and 43% compared with RSV seasons before the COVID-19 pandemic. Pediatric RSV immunizations will likely have similar effectiveness against hospitalization during the 2025-2026 respiratory season as they have in past years.
For adults, ACIP recommends a single lifetime dose of RSV vaccine for all adults aged 75 years and older and adults aged 50-74 years with high-risk conditions. Adults who have received the vaccine since it became available in 2023 are still expected to have vaccine-derived immunity moving into the 2025-2026 season. Among adults 75 years and older, RSV vaccine coverage increased from 28.8% to 47.5% over the course of the 2024-2025 season. We note uncertainty in how many more eligible adults will seek out vaccination this season. In studies of the real-world effectiveness of two of the currently available RSV vaccines during the 2023–2024 RSV season, vaccines effectively reduced the likelihood of RSV-associated hospitalizations and emergency department visits in adults 60 and older during the same season as vaccine receipt. Adult RSV vaccine effectiveness is expected to vary with time since vaccination, with lower effectiveness in people who received the vaccine in a prior season, because immunity may wane over time.
Key methods
This outlook is based on expert opinion and historical data for COVID-19, influenza, and RSV with the addition of scenario modeling for COVID-19. We have low to moderate combined confidence in our assessment, based on information availability and information gaps and assumptions.
This respiratory outlook incorporates expert opinion from 20 subject-matter experts specializing in COVID-19, influenza, and RSV epidemiology, infectious disease modeling, disease surveillance, and risk assessment methods, including several experts from Insight Net. In partnership with Metaculus, CDC designed a questionnaire and expert elicitation process for soliciting views from experts on the upcoming fall and winter respiratory season. Experts each answered a series of questions on the expected hospitalization burden posed by each disease, as well as on key drivers for a season with a higher peak hospitalization rate. Experts assigned confidence levels to their answers as a way of reflecting their uncertainty in their response. The results were used to inform this outlook and as inputs into scenario modeling. See our expert elicitation methods for further information on this process.
Scenario modeling methods
Scenario modeling explores longer-term hypothetical outcomes under different assumptions about the future. Our COVID-19 scenario modeling utilizes a transmission model with a compartmental modeling structure that takes into account population age structure, infection history, vaccination history, immunity waning status, and infecting strain. Immunity is determined by immunogenic events (infections and vaccinations) and time since the most recent event. Protection against infection is strain-specific: past infection with a more similar variant, or vaccination with a better-matched vaccine, provides a higher level of protection against the challenging strain. The model uses mathematical equations to describe how groups move between compartments (e.g., from uninfected to infected, or from unvaccinated to vaccinated). See our Behind the Model to learn more about how scenario modeling can be used to inform decision-making.
Both scenarios presented here assume that only people over the age of 65 and those with underlying health conditions will receive a COVID-19 vaccine in the 2025-2026 season. In the model, the 65+ age group receives vaccines at the same rate as in 2024-2025. A proportion of 18- to 64-year-olds equivalent to the proportion of the population with relevant underlying conditions ("high risk" groups) also receive vaccination at the same rate as in 2024-2025. We also assume vaccine effectiveness is the same as in 2024-2025.
The two sets of projections shown consider different possible emergence scenarios for COVID-19 variants. In Scenario A, it is assumed that no variant will emerge that significantly evades the population's immunity. In Scenario B, a variant with moderate immune escape properties emerges in November. Under this scenario, people in the model experience a small risk of exposure to the new variant that increases gradually over two weeks, peaks on November 1, and then decreases over two weeks. We assume that this variant has similar properties to the variants that were dominant during the summer 2024 and winter 2024-2025 waves.
Appendix
- We chose to introduce a variant with moderate immune-escape properties in November to align with the timing of variant introduction during the 2024-2025 respiratory season. The variant is introduced by creating a small risk of exposure for people in the model that increases gradually over two weeks, peaks on November 1, and then decreases over 2 weeks.