At a glance
These instructions are in accordance with CDC regulations and are for the use of panel physicians evaluating persons applying for immigrant or refugee status, as well as certain non-immigrants who are required to have an overseas medical examination. These instructions focus on physical or mental disorders with associated harmful behaviors and substance use disorders.
Background
The purpose of the immigration examination is to identify health-related conditions that render an applicant inadmissible (Class A). The Immigration and Nationality Act (INA) provides three grounds of inadmissibility related to substance addiction or abuse, or physical or mental disorders that affect behavior. They are:
- Current physical or mental disorder with associated harmful behavior.
- Current physical or mental disorder with a history of associated harmful behavior if the harmful behavior is likely to recur or lead to other harmful behavior in the future.
- Drug (substance) abuse or addiction (medically identified as a "substance use disorder") of any of the substances listed in Section 202 of the Controlled Substances Act (Appendix C).
Thus, medical screening for physical and mental disorders with associated harmful behaviors and substance use disorders among persons applying for adjustment of status in the U.S. is an essential component of the immigration process. Because such conditions are challenging to diagnose and treat, these Technical Instructions provide a method for recording findings from the medical examination and guidance for the panel physician on classifying applicants. The Technical Instructions use uniform criteria for diagnosis consistent with current medical knowledge and standards of the American Psychiatric Association's Diagnostic and Statistical Manual of Mental Disorders Fifth Edition, Text Revision (DSM-5-TR).
The instructions in this document supersede all previous Mental Health Technical Instructions, updates to the Technical Instructions, memoranda and letters to panel physicians, and memoranda and letters to international refugee resettlement organizations.
For questions about these Technical Instructions, please contact the Immigrant and Refugee Health Branch of the Division of Global Migration Health (DGMH), Centers for Disease Control and Prevention (CDC), at panelphysicans@cdc.gov. For more information pertinent to these instructions and the required medical examination for applicants for U.S. immigration, visit: Technical Instructions for Panel Physicians.
Key Concepts
"V" Coded Condition
"V" coded conditions listed in the DSM are not diagnoses but are used in clinical practice settings when the focus is on a behavior that is not due to a mental disorder. Because "V" coded conditions are not mental disorders, they cannot be used in determining if a person has an inadmissible (Class A) health-related condition, regardless of whether there is an associated harmful behavior. However, treatment might be recommended for behaviors associated with "V" coded conditions.
Physical Disorder
Physical disorders are clinically diagnosed medical conditions where the focus of attention is physical manifestations. Only physical conditions that are included in the current version of the International Classification of Diseases (ICD) will be considered for the purpose of this portion of the overseas examination.
Physical disorders are rarely associated with harmful behavior. However, it may happen in delirious or confused states due to metabolic disturbances, hypoglycemia, some psychomotor epilepsies and in the aftermath of generalized seizure disorders.
Physical disorders that have associated harmful behaviors, either current or likely to recur, are inadmissible (Class A) conditions.
Physical disorders that do not have associated harmful behaviors or that have a history of associated harmful behaviors that have been judged unlikely to recur are considered Class B conditions.
Mental Disorder
Mental disorders are health conditions that are characterized by alterations in thinking, mood, or behavior (or some combination). The current version of the DSM is an authoritative source on the classification of mental disorders and must be followed for this portion of the overseas medical examination. For the purposes of these Technical Instructions, "mental disorders" do not include substance use disorders. Substance use disorders are addressed separately, below.
Mental disorders that have associated harmful behaviors, either current or likely to recur, are inadmissible (Class A) conditions.
Mental disorders that do not have associated harmful behaviors or that have a history of associated harmful behaviors that have been judged unlikely to recur are considered Class B conditions.
Substance Use Disorder
The DSM diagnosis for substance use disorders is used in this portion of the overseas medical examination to determine "drug abuse" and "drug addiction."
The essential feature of a substance use disorder is a cluster of cognitive, behavioral, and physiological symptoms indicating that the individual continues using the substance despite significant substance-related problems. Diagnosis of substance use disorders are to be made in accordance with existing medical standards as determined by the current edition of the DSM. There are 11 criteria for substance use disorders listed in the DSM, grouped into four primary categories: impaired control, social impairment, risky use, and physical dependence. A detailed list of and additional commentary on the 11 criteria for substance use disorders can be found in the DSM-5. The panel physician must assess each of the 11 criteria in determining whether an individual has (or has ever had) a substance use disorder and at least 2 criteria must be met in order to make a diagnosis. In other words, if an applicant's substance use does not meet at least 2 of the DSM substance use disorder criteria, they are considered "No Class."
For the purpose of this evaluation, substances will be considered as belonging to one of the two following categories:
- Controlled substances Act (CSA) substances - include any substance listed in Schedules I through V of Section 202 of the CSA. (See Appendix C.) Substance use disorders (of any severity) involving a CSA substance are inadmissible (Class A) conditions and do not require additional evidence of associated harmful behavior.
- Non-CSA substances - include alcohol and all other psychoactive substances not found in the CSA. Substance use disorders (of any severity) involving a non-CSA substance must also be assessed for associated harmful behavior. Those with associated harmful behaviors, either current or likely to recur, are inadmissible (Class A) conditions. Those without any associated harmful behaviors are considered Class B conditions and are not inadmissible.
Harmful Behavior
A harmful behavior is defined as an action associated with a mental or physical disorder, or a non-CSA substance use disorder that is causing or has caused any of the following:
- Serious psychological or physical injury to the applicant or to others (e.g., a suicide attempt or child abuse).
- A serious threat to health or safety (e.g., driving while intoxicated or verbally threatening to kill someone).
- Major property damage.
Mental disorders most associated with harmful behavior include:
- Mood disorders.
- Anxiety disorders that include post-traumatic stress disorder, panic disorders, and phobias.
- Personality disorders that include antisocial, paranoid, and borderline personality disorders.
- Sexual disorders that include paraphilia.
- Schizophrenia and other psychotic disorders.
However, the following are excluded from the above definition of "harmful behavior" for the purpose of this examination:
- Harmful behaviors that are the direct result of an applicant's environment - if the harmful behavior would likely cease completely if the applicant was removed from the current environment (e.g., an abusive household or a region in which they are persecuted), that harmful behavior is not considered for the purposes of these instructions.
- Nonsuicidal self-injury - if it is determined that the harmful behavior is being inflicted toward the applicant themselves and is not life threatening or indicating an intent to die, but rather an attempt to cope with emotional pain, sadness, anger and stress (e.g., superficial cutting, scratching, burning), that harmful behavior is not considered for the purpose of these instructions.
- Harmful behaviors resulting from an applicant's significant intellectual disability (regardless of the cause) - if the harmful behavior is done as a means of expressing frustration, such as hitting, biting or head-banging and not with any intent to harm, that harmful behavior is not considered for the purpose of these instructions.
Thus, for the remainder of this document, the term "harmful behavior" is referring only to those behaviors that meet the above definition, applying the listed exclusions.
As discussed above, a CSA substance use disorder alone is an inadmissible condition (Class A) and does not require the additional presence of harmful behavior to be considered inadmissible.
Applicants with harmful behaviors not associated with a physical or mental disorder or a non-CSA substance use disorder may be rendered inadmissible under criminal grounds as determined by [an adjudicating officer of] the U.S. Citizenship and Immigration Services (USCIS) or the Department of State (DOS). However, only harmful behaviors associated with a physical or mental disorder or non-CSA substance use disorder are relevant for the determination of medical ineligibility; neither harmful behavior nor the physical or mental disorder or non-CSA substance use disorder alone makes an applicant medically inadmissible.
Mental Health Examination
Overview
As part of the history and physical examination of the applicant, the panel physician must:
- Identify and diagnose any physical or mental disorders, or substance use disorders.
- Identify any harmful behavior associated physical or mental disorders or non-CSA substance use disorders.
- Determine the likelihood of recurrence of prior harmful behaviors.
- Determine the remission status of any disorder previously diagnosed.
For most applicants, this can be completed in one appointment. However, for some applicants, multiple appointments or consultations with a mental health specialist may be needed to make an accurate diagnosis (see referral section below).
Medical History and Psychiatric Evaluation
The panel physician should obtain and consider as much information as possible regarding the applicant's medical and behavioral history. At a minimum, the panel physician should do the following:
- Complete a thorough history to include (but not limited to) questions about:
- The applicant's history of diagnosed mental or physical disorders.
- The applicant's use of CSA and non-CSA substances and prescription medicines, both currently and in the past.
- The applicant's current or past behaviors that are or were harmful to self or others.
- Conduct an activities assessment and mental status examination that assess at a minimum:
- Orientation
- Mood and affect
- Speech and language
- Thought process and content
- Behavior
- Review other relevant records (if available), such as police, military, school, and employment, and any historical medical records, that might provide a history of harmful behavior or substance use.
- Ask family members for information about the applicant regarding social dysfunction, as well as any school, occupational or law enforcement problems.
If any associated harmful behaviors are identified, the panel physician should then do the following:
- Determine whether the behavior is current or in the past.
- Decide whether any past harmful behavior is unlikely to recur. Past harmful behavior is considered unlikely to recure if both of the following are true:
- The underlying physical or mental disorder or non-CSA substance use disorder is either in remission or is reliably controlled by medication or other effective treatment; AND
- It has been at least 12 months since the harmful behavior occurred. However, clinical judgement must be used to determine if this is enough time to make a decision (see "Remission" section).
Under most circumstances, applicants will not require additional psychological or neuropsychological testing. Projective instruments, such as the Rorschach test, may not be useful given the added administrative and time burden; however, particularly when harmful behavior is present, these tests may be used to aid in making a diagnosis.
For applicants who demonstrate cognitive impairment such as dementia or intellectual disability, the panel physician may estimate the degree of impairment by assessing the applicant's (1) level of knowledge and (2) ability to carry out functions of daily living (e.g., learning, communication, and routine activities). Any available reports of cognitive, development, intelligence testing, or neuropsychological testing in the medical record should be included with the panel physician's report. However, the panel physician is not required to routinely send such applicants for additional psychological tests and should not do so unless a medical inadmissibility is suspected.
Laboratory Testing for Substances
The panel physician should not routinely subject whole populations of applicants to laboratory testing such as urine drug testing. Instead, the panel physician must evaluate the individual applicant's history, behavior and physical appearance when determining if laboratory testing should be performed. (see Table 1)
However, there are two circumstances in which laboratory testing for CSA substances is required as part of the mental health examination:
- When a panel physician defers a diagnosis or classification of a CSA substance use disorder for 3 to 6 months, random laboratory testing for CSA substances on short notice (i.e., 24 to 48 hours after notification) to the applicant is required to aid in the determination of diagnosis and classification. Panels must perform a minimum of three tests during the 3-to-6-month period.
- When determining remission from a CSA substance use disorder, random laboratory testing for CSA substances on short notice (i.e., 24 to 48 hours after notification) to the applicant is required to aid in this determination by confirming the absence of substance use. Panels must perform a minimum of four tests over a 12-month period.
If laboratory testing for the CSA substance associated with the substance use disorder is not routinely available in the country, please contact panelphysicians@cdc.gov for additional instruction.
Laboratory testing for alcohol use disorders is largely non-specific and as such, panel physicians are not permitted to use these tests in place of standard diagnostic screening tools. However, laboratory testing can be used along with clinical judgement as an additional piece of clinical information to confirm a suspected diagnosis and to document remission for alcohol use disorders (see remission section below). Although not required for the medical examination, several laboratory alcohol "biomarkers" can be used including:
- Liver enzymes: a ratio of aspartate aminotransferase (AST): alanine aminotransferase (ALT)>2:1 is suggestive of alcohol-induced liver disease.
- Gamma-glutamyltransferase (GGT): elevated levels can suggest excessive alcohol use. GGT levels of >30U/IL can reflect alcohol consumption of >4 drinks per day.
- Carbohydrate-deficient transferrin (CDT): considered more specific than GGT alone for chronic excessive alcohol use with few factors causing false positives. It can be used to distinguish heavy alcohol use from social drinking. When used in combination, GGT-CDT, can further improve the detection of excessive alcohol consumption.
- Urine test for alcohol metabolites: ethyl glucuronide (EtG) and ethyl sulfonate (EtS) are minor metabolites of ethanol and be detected for up to 5 days in urine, although these tests will have higher accuracy for the first 24 hours after use. Test sensitivity is highest in heavy drinkers.
- Blood alcohol levels: generally used for detecting acute alcohol intoxication and thus may have limited utility for the medical examination.
Other laboratory testing depends on the availability of laboratory services and the clinical judgment of the panel physician. For instance, laboratory testing to identify underlying medical conditions causing psychiatric manifestations may be necessary before making any diagnoses. However, specialized laboratory testing, such as dexamethasone suppression tests or challenge administration of various pharmaceuticals, is usually not indicated.
Therapeutic levels of prescribed anticonvulsant medications, antipsychotic medications, or other medicines used in psychiatry (such as lithium levels) might also be of value to the panel physician or mental health specialist in:
- Determining the applicant's adherence to a prescribed course of treatment.
- Possibly changing or adjusting the applicant's medication, and therefore contributing to remission of illness and reduction of associated harmful behavior.
Panel physicians must know the reliability and validity of the laboratory tests and laboratory methods used during the medical evaluation. All laboratory testing for substances must be done using materials licensed by the U.S. Food and Drug Administration or by the equivalent licensing office in the country where the examination is being performed. Rapid testing or semi-quantitative testing may be used for the screening test; however, gas chromatography/mass spectrometry (GC/MS), performed at a reference laboratory, must be used as the confirmatory test. Positive and negative controls must be used with any testing and only test kits that are for medical diagnosis and treatment must be used. Forensic testing is minimally regulated and will be labeled "not for medical diagnosis and treatment." Therefore, it should not be used because it is not sensitive enough for medical purposes.
Referring the Applicant to a Specialist
Referral to a mental health specialist is not a requirement for this examination. However, after reviewing the applicant's medical history and performing a psychiatric evaluation, the panel physician might feel that a more specialized psychiatric examination is indicated to determine if an applicant has a mental or physical disorder with associated harmful behavior, or a substance use disorder involving a CSA or non-CSA substance (See Table 2). In these cases, the panel physician should have a previously identified mental health specialist who can carry out a full psychiatric evaluation. Panel physicians should only refer cases to a specialist to confirm or rule out a suspected inadmissibility (Class A condition) and only when the panel physician is unable to make a diagnosis or determination regarding associated harmful behavior utilizing their own level of expertise.
Virtual evaluations by a mental health specialist are acceptable for this portion of the mental health examination only and no other portion of the U.S. Immigration Medical Examination
Deferring a Diagnosis/Classification
If the panel physician is unable to determine whether an applicant has an inadmissible (Class A) condition, the panel physician may defer diagnosis and classification for 3 to 6 months to obtain additional medical evidence.
As noted above, in cases where a diagnosis or classification is deferred for a suspected CSA substance use disorder, random testing for substances on short notice to the applicant is required to aid in the determination of diagnosis and classification. Panels must perform a minimum of three tests during this period.
In cases of deferment for a suspected mental or physical disorder or non-CSA substance use disorder with associated harmful behavior, panels may use this time to obtain additional records, communicate with family members, obtain relevant laboratory testing, or refer to a specialist for a more detailed evaluation.
For applicants with deferred diagnosis and classification, the panel physician must have medical rationale for the deferment and must clearly explain to the applicant what is required during the next 3 to 6 months for the panel physician to be able to diagnose and classify. Panel physician should also ideally write these instructions in a document that is signed by the applicant.
Referring a Case to DGMH
If an applicant has been referred to a mental health specialist for psychiatric evaluation and the panel physician still needs assistance in determining the diagnosis and classification of a suspected inadmissibility (Class A condition), DGMH may be consulted to provide additional assistance.
Panel physicians should only consult DGMH in situations where, after their own examination and evaluation by a mental health specialist, they are still unable to make a final determination on diagnosis or classification.
To submit a case to DGMH for review, send a copy of all pertinent medical information via secure files to panelphysicians@cdc.gov.
Remission
Remission must be considered in three contexts (see Figure 2):
- General mental or physical disorders
- CSA-substance use disorders
- Non-CSA substance use disorders (e.g. alcohol disorders)
For general mental and physical disorders, the determination of remission must be made based on both of the following criteria:
- The disorder must be under control by one or more of the following: medication, therapy or natural history of the disorder; AND
- It has been at least 12 months since the last occurrence of associated harmful behavior.
For CSA substance use disorders, the determination of remission must be made based on both of the following criteria:
- At least 12 consecutive months during which the applicant does not meet any DSM criteria for a substance use disorder, with the exception of craving; AND
- Full abstinence from use. Abstinence must be verified by a minimum of four random laboratory screenings on short notice for CSA substances over a 12-month period. If laboratory testing for the CSA substance associated with the substance use disorder is not routinely available in the country, please contact panelphysicians@cdc.gov for additional instruction.
- The 12 months of sustained remission can begin prior to the immigration medical exam if the panel physician can document the applicant's remission efforts. This requires corroborating the applicant's responses with input from family members, therapists, support groups, rehabilitation facilities, etc. and documentation of at least one negative random laboratory screen. Otherwise, the 12 months of sustained remission begins at the first negative laboratory screen performed as part of the immigration medical exam.
- When used for achieving sustained remission of an opioid use disorder, agonist therapy such as methadone or buprenorphine, should not be considered a CSA substance.
For non-CSA substance use disorders (e.g. alcohol use disorders), full abstinence from use is not required to determine remission. However, in lieu of full abstinence, both of the following must be met:
- At least 12 consecutive months during which the applicant does not meet any DSM criteria for a substance use disorder, except craving. The panel physician must document their efforts to corroborate the applicant's responses with input from the family members, therapists, support groups, rehabilitation facilities, etc.; AND
- At least 12 months since the last occurrence of associated harmful behavior.
- The 12 months of sustained remission can begin prior to the immigration medical exam if the panel physician can document the applicants' remission efforts. This requires corroborating the applicant's responses with input from family members, therapists, support groups, rehabilitation facilities, etc. Otherwise, the 12 months of sustained remission begins at the time of the immigration exam.
For alcohol use disorders, although not required, some laboratory monitoring can be useful to confirm a reduction in use. See the above laboratory section for more details.
If an applicant claims to have previously met the above listed criteria for remission from any Class A disorder, but has no objective documentation to corroborate their account, the panel physician must defer for 3-6 months and follow the requirements outlined in the "deferring a diagnosis/classification" section above.
Class A Applicants
All applicants with Class A conditions for physical or mental disorders and substance use disorders should be reported to the U.S. Embassy upon detection.
Panel physicians can tell applicants their final diagnosis (e.g., major depression with harmful behavior); however, only the Department of State can tell applicants they are inadmissible (Class A). After applicants receive notification from the Department of State and are referred back to the clinic, panel physicians must explain what is expected for them to meet criteria for remission. If treatment is indicated, panel physicians should also provide information regarding recommended treatment options. Panel physicians should ideally write these instructions in a document that is signed by the applicant.
Applicants who have been determined to be Class A for a substance use disorder involving a CSA substance are not eligible for a waiver (see "Waivers" section below for more information) and therefore, must complete the required criteria for remission before reapplying for admission. However, under section 207 of the INA, USCIS may waive this provision if the applicant is seeking admission to the United States as a refugee.
Additional Concepts to Consider
Marijuana (i.e., Tetrahydrocannabinols (THC))
Despite several U.S. state governments legalizing marijuana or some of its derivatives, including derivatives with > 0.3% THC, it is still considered a CSA substance by the United States Drug Enforcement Agency (DEA).
As is true for all CSA substances, applicants' admitting occasional use or having one positive urine drug test alone does not make an applicant inadmissible (Class A). To be considered Class A, they must meet at least 2 of the 11 DSM criteria for a substance use disorder. The topics of deferment, remission, and laboratory testing for CSA substances are detailed above.
Prescription Drugs
Substances used for clinical care in medical practice are not prohibited. Prescription drugs taken in accordance with a prescription do not amount to a substance use disorder. However, misuse of prescription drugs could indicate a substance use disorder. If that is suspected, further investigation would require a full evaluation by the examining physician with particular attention to whether illicit drugs are being used, because use of illicit drugs is a risk factor for the abuse of prescribed CSA substances.
Sexually Dangerous People
Not all sexually dangerous people have behaviors attributable to a mental disorder. Likewise, not all people diagnosed with a paraphilic disorder will demonstrate harmful behavior. As stated in the Mental Disorder and Harmful Behavior sections above, there must be an underlying diagnosable mental disorder with associated harmful behavior - either current, or likely to recur - to be considered a Class A condition. Of note, harmful behaviors do include the viewing of child pornography because children are at least indirectly harmed, or at worst directly harmed, during the making of such imagery.
To achieve remission for a Class A paraphilic disorder, applicants must still meet the same remission criteria outlined above for other mental disorder, with the exception of pedophilic disorder. Research has demonstrated that individuals diagnosed with pedophilic disorder do not reliably benefit from treatment programs and thus can never truly reach a point where there is no risk that they will act on their desires. As a result, remission for pedophilic disorder is not achievable and any applicant diagnosed with pedophilic disorder must remain medically classifiable as Class A for the remainder of their lives.
Screening Results and Classifications
The mental health screening is complete when all required aspects of the medical examination have been finalized, including the report of the specialist and laboratory test results, if indicated.
Applicants may have more than one classification. For instance, an applicant can be Class A for both a mental disorder and a CSA substance use disorder. However, applicants cannot be classified as both Class A and Class B for the same physical, mental disorder, or substance disorder.
Screening Results and Classifications
There are three categories of mental health and substance use disorder classifications, listed below:
No Class A or Class B Classification
- Applicants with no diagnosis of physical or mental disorder.
- Applicants with occasional use of a substance (CSA or non-CSA), but who do not meet criteria for substance use disorder.
- Applicants with harmful behavior that is not associated with any diagnosable physical or mental disorder, or substance use disorder.
Class A Classification
- Applicants diagnosed with current physical or mental disorder with associated harmful behavior.
- Applicants diagnosed with a non-CSA substance use disorder (e.g. alcohol use disorder) with associated harmful behavior.
- Applicants diagnosed with a CSA substance use disorder
Class B Classification
- Applicants diagnosed with current physical or mental disorder with no associated harmful behavior.
- Applicants diagnosed with a non-CSA substance (e.g. alcohol use disorder) without a history of associated harmful behavior.
- Applicants diagnosed with physical or mental disorder with a history of associated harmful behavior, now in remission.
- Applicants diagnosed with a CSA substance use disorder now in sustained remission.
- Applicants diagnosed with a non-CSA substance use disorder with a history of associated harmful behavior, now in remission.
DSM Diagnoses and Classification
| Substance Use Disorder | ||||
|---|---|---|---|---|
| Involves CSA Substance | Associated Harmful Behaviors (current, or likely to occur) | Meets Criteria for Remission | Classification | Corresponding Classification on DS Forms |
| Yes | N/A | No | CLASS A: CSA Substance Use Disorder | CLASS A: Addiction or abuse of a specific substance on the CSA |
| Yes | CLASS B: CSA Substance Use Disorder, in remission | CLASS B: Sustained, full remission of addiction or abuse of specific substance on the CSA | ||
| No | Yes | No | CLASS A: Non-CSA Substance Use Disorder, with associated harmful behavior | CLASS A: Any physical or mental disorder (including other substance-related disorder) with harmful behavior or history of such behavior likely to recur |
| Yes | CLASS B: Non-CSA Substance Use Disorder, with history of associated harmful behavior, in remission | CLASS B: Any physical or mental disorder (excluding addiction or abuse of specific substance on the CSA but including other substance-related disorder) without harmful behavior or history of such behavior unlikely to recur | ||
| No | N/A | CLASS B: Non-CSA Substance Use Disorder, without associated harmful behavior | CLASS B: Any physical or mental disorder (excluding addiction or abuse of specific substance on the CSA but including other substance-related disorder) without harmful behavior or history of such behavior unlikely to recur | |
| Mental or Physical Disorder | |||
|---|---|---|---|
| Associated Harmful Behaviors (current, or likely to occur) | Meets Criteria for Remission | Classification | Corresponding Classification on DS Forms |
| Yes | No | CLASS A: Mental or physical disorder, with associated harmful behavior | CLASS A: Any physical or mental disorder (including other substance-related disorder) with harmful behavior or history of such behavior likely to recur |
| Yes | CLASS B: Mental or physical disorder, with a history of harmful behavior unlikely to recur | CLASS B: Any physical or mental disorder (excluding addiction or abuse of specific substance on the CSA but including other substance-related disorder) without harmful behavior or history of such behavior unlikely to recur | |
| No | N/A | CLASS B: Mental or physical disorder, without associated harmful behavior | CLASS B: Any physical or mental disorder (excluding addiction or abuse of specific substance on the CSA but including other substance-related disorder) without harmful behavior or history of such behavior unlikely to recur |
Waivers
Applicants with a Class A physical or mental disorder or non-CSA substance use disorder with associated harmful behavior can petition for a Class A waiver. The applicant should complete Form I-601 or I-602 (for immigrants or refugees, respectively) and submit directly to USCIS. After submission, DGMH reviews the waivers and supporting medical examination upon request by USCIS to provide an opinion regarding the case. DGMH's review of the waiver and supporting medical examination documentation ensure the applicant has been classified properly and that an appropriate U.S. health care provider is identified for the applicant to continue treatment post arrival. However, only USCIS has the final authority to adjudicate the waiver request.
Immigrant visa applicants diagnosed with CSA substance use disorders are not eligible for a waiver. However, under section 207 of the INA, the USCIS may waive this provision if the applicant is seeking admission to the U.S. as a refugee.
Documentation
Panel physicians should indicate pertinent information relating to physical or mental disorders and substance use disorders on the DS-3026 or 501 Medical Examination in eMedical and assign any Class A or B classifications on the DS-2054 or in the 106 Mental Health Report in eMedical.
For applicants who are referred to a mental health specialist for psychological or laboratory testing, the panel physician is required to attach the original specialist's report or the testing result to the DS forms or upload to eMedical. The report from the specialist and all testing results must be provided in English.
For applicants evaluated for a substance use disorder, the panel physician or mental health specialist is required to clearly document which of the 11 DSM criteria were met and include this in their report.
The panel physician should attach to the DS forms or upload into the eMedical record any other documents provided for review regarding diagnosis or classification of a physical or mental disorder, or substance use disorder for an applicant.
Incomplete documentation may result in refusal to grant a visa or designation of medical hold status at arrival to ports of entry.
Appendices
Appendix A: Glossary of Abbreviations
Acronym
Full Phrase
CDC
Centers for Disease Control and Prevention, United States
DGMH
Division of Global Migration Health
DHS
Department of Homeland Security
DSM
Diagnostic and Statistical Manual of Mental Disorders
ICD
Manual of the International Classification of Diseases
USCIS
United States Citizenship and Immigration Services
Appendix B: Useful Resources
American Psychiatric Association: Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition. Diagnostic and Statistical Manual of Mental Disorders | Psychiatry Online
Appendix C: Controlled Substances
Schedules I through V of Section 202 of the Controlled Substances Act. Found in Part 1308 of Title 21 Code of Federal Regulations.
Figures
Figure 1: Classification Algorithm for Suspected Substance Use Disorder, or Physical or Mental Disorder
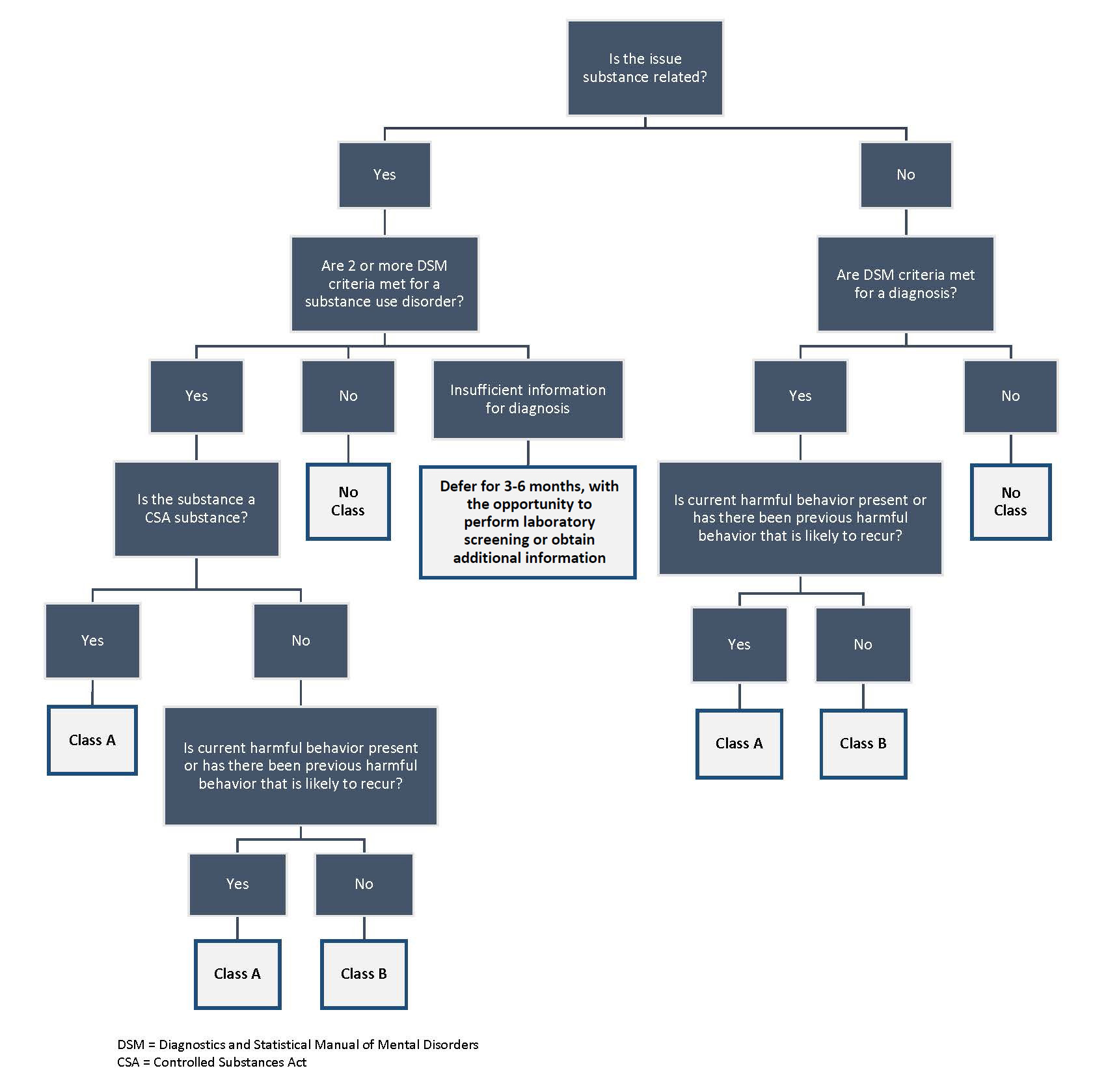
Figure 2. Classification Algorithm for Evaluating Remission after a Class A Determination

Tables
Table 1. Indications for Laboratory Drug Screening
Include (but are not limited to):
- History of any substance abuse or dependence with a specific substance listed in Schedules I through V of Section 202 of the Controlled Substances Act. (See Appendix C).
- Applicant-provided information that appears to contradict information provided by family members or from other records such as police, military, school and employment.
- Unexplained gaps of time in the applicant's past schooling or employment.
- Evidence of unreliable or false information given during the interview or examination.
- Any demeanor, presentation, or findings that the examining physician associates with substance abuse or dependence, such as motor ability and interpersonal skills; deepened skin coloring, needle scarring, or skin ulcers along the veins in the arms or legs; a hard or bumpy liver.
- Evidence or appearance of intoxication with any substance during the examination; disturbed behavior that might be associated with a substance-related disorder.
- Follow-up of an initial positive drug screen.
- Monitoring remission.
- Deferring diagnosis/classification after confirmed or suspected substance use.
Table 2. Referring Applicant to a Mental Health Specialist
The panel physician may refer the applicant to a mental health specialist if after interview, review of records, and examination, they are unable to:
- Arrive at a probable diagnosis of a current mental disorder with associated harmful behavior.
- Arrive at a probable diagnosis of current CSA substance use disorder according to DSM criteria.
- Arrive at a probable diagnosis for past episodes of mental disorder or determine that previous difficulties in functioning were the result of a mental disorder that is associated with harmful behavior.
- Rule out the presence of a mental disorder that may be associated with harmful behavior.
- Determine if harmful behavior has been associated with a physical or mental disorder.
- Determine if harmful behavior has been associated with a known non-CSA substance use disorder.
- Determine if any prior associated harmful behavior is likely to recur.
- Determine if any diagnosed physical or mental disorders that were associated with harmful behavior are under control.
- Determine if any diagnosed non-CSA substance use disorders that were associated with harmful behavior are in remission.
- Determine if any diagnosed CSA substance use disorders are in remission.
- Determine the likelihood of maintaining remission or effective control of diagnosed physical or mental disorders that affect behavior.