What to know
- Maternal Mortality Review Committees (MMRCs) are multidisciplinary committees that convene at the state or local level to comprehensively review deaths during or within a year of pregnancy (pregnancy-associated deaths). MMRCs have access to clinical and non-clinical information (e.g., vital records, medical records, social service records) to more fully understand the circumstances surrounding each death, determine whether the death was pregnancy-related, and develop recommendations for action to prevent similar deaths in the future.
- Purpose: This page contains a description of the MMRC data, methods for variable creation, and definitions of select variables.
About the system
The Maternal Mortality Review Information Application (MMRIA, pronounced "Maria") is a CDC data system designed to facilitate MMRC functions through a common data language. MMRIA supports standardized record abstraction, case summary development, documentation of committee decisions, and analysis. All states and territories across the United State can use MMRIA.
Jurisdictional MMRCs shared data with CDC for aggregate analysis through MMRIA. In some states, only partial years of data were shared and not every jurisdiction shared all years of data. Some states group review of deaths by cause of death and may have only reviewed some causes before sharing data with CDC. Sensitivity analysis did not indicate any major differences in underlying causes of death when data for those states were excluded.
Data sources
Data analyzed included information on pregnancy-related deaths that occurred during 2017–2019 among residents of 36 states: Alabama (2017–2018), Alaska (2019), Arizona (2017–2019), Arkansas (2018–2019), California (2019), Colorado (2017–2019), Connecticut (2017–2019), Delaware (2017–2019), Florida (2017–2019), Georgia (2017–2018), Hawaii (2017–2018), Illinois (2017–2019), Indiana (2017–2019), Kansas (2017–2019), Louisiana (2017–2019), Massachusetts (2017), Minnesota (2017–2018), Mississippi (2017–2019), Missouri (2017–2019), North Carolina (2018–2019), Nebraska (2017–2019), New Hampshire (2017–2019), New Jersey (2017–2019), New Mexico (2017–2019), New York (2018–2019; 2019 excludes NYC), Ohio (2017–2018), Oklahoma (2017–2019), Oregon (2018–2019), Pennsylvania (2018), Tennessee (2017–2019), Texas (2019), Virginia (2018), Washington (2017–2019), West Virginia (2017–2019), Wisconsin (2017), and Wyoming (2018–2019).
Data analyzed included information on pregnancy-related deaths that occurred in 2020 among residents of these 38 states: Alabama, Alaska, Arizona, Arkansas, California, Colorado, Connecticut, Delaware, Florida, Georgia, Illinois, Indiana, Iowa, Kansas, Kentucky, Louisiana, Maryland, Massachusetts, Michigan, Minnesota, Mississippi, Missouri, Montana, Nebraska, New Hampshire, New Jersey, New Mexico, New York, Ohio, Oklahoma, Oregon, Pennsylvania, Rhode Island, Tennessee, Utah, Washington, Wisconsin, and Wyoming.
Data analyzed included information on pregnancy-related deaths that occurred in 2021 among residents of these 46 states: Alabama, Alaska, Arizona, Arkansas, California, Colorado, Connecticut, Delaware, Florida, Georgia, Hawaii, Idaho, Illinois, Indiana, Iowa, Kansas, Kentucky, Louisiana, Maine, Maryland, Massachusetts, Michigan, Minnesota, Mississippi, Missouri, Montana, Nebraska, New Hampshire, New Jersey, New Mexico, New York, North Carolina, Ohio, Oklahoma, Oregon, Pennsylvania, Rhode Island, South Carolina, South Dakota, Tennessee, Utah, Virginia, Washington, West Virginia, Wisconsin, and Wyoming.
How information is categorized
Classification of pregnancy-related deaths among American Indian or Alaska Native Women
Methodological decisions about racial classification can affect the size and characteristics of the population used in an analysis. Assessments from other groups123 have demonstrated the importance of examining pregnancy-related deaths among all American Indian or Alaska Native (AI/AN) women, regardless of notation of Hispanic origin or other/multiple races. We used an approach which classifies non-Hispanic single-race AI/AN, and AI/AN in combination with any other race or ethnicity as American Indian or Alaska Native.
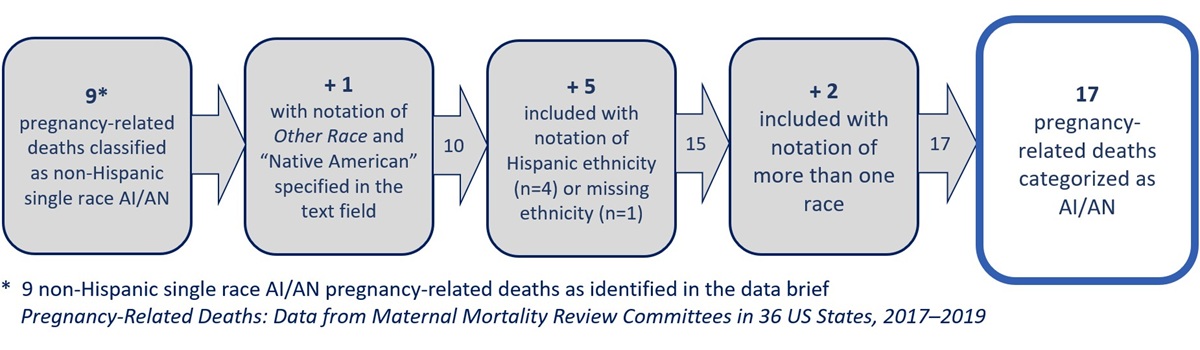
In the 2017 - 2019 MMRIA data, 9 pregnancy-related deaths were classified as non-Hispanic single-race AI/AN. As shown in Figure 1, by using an alternate approach to classifying available vital records information on race and ethnicity, 17 pregnancy-related deaths were classified as AI/AN. Because of known limitations of vital records data for identifying AI/AN women4, 17 is still likely an undercount of deaths among AI/AN women.
Figure 1. Classification of pregnancy-related deaths among American Indian or Alaska Native in Data from MMRCs in 36 US States, 2017–2019
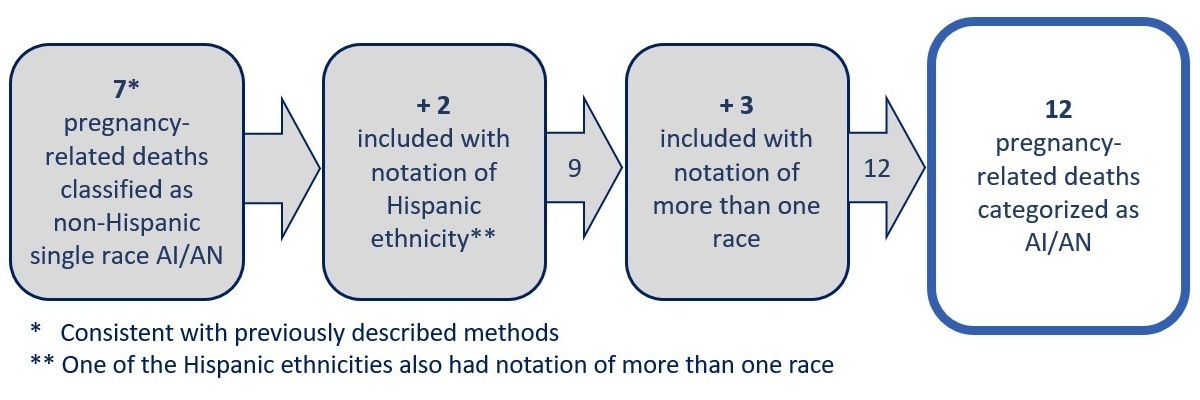
In the 2020 MMRIA data, 7 pregnancy-related deaths were classified as non-Hispanic single-race AI/AN. As shown in Figure 2, by using an alternate approach to classifying available vital records information on race and ethnicity, 12 pregnancy-related deaths were classified as AI/AN.
While this alternate approach resulted in the increased identification of pregnancy-related deaths among AI/AN women, because of known limitations of vital records data for identifying AI/AN women4, 12 is still likely an undercount of deaths among AI/AN women.
Figure 2. Classification of pregnancy-related deaths among American Indian or Alaska Native in Data from MMRCs in 38 US States, 2020
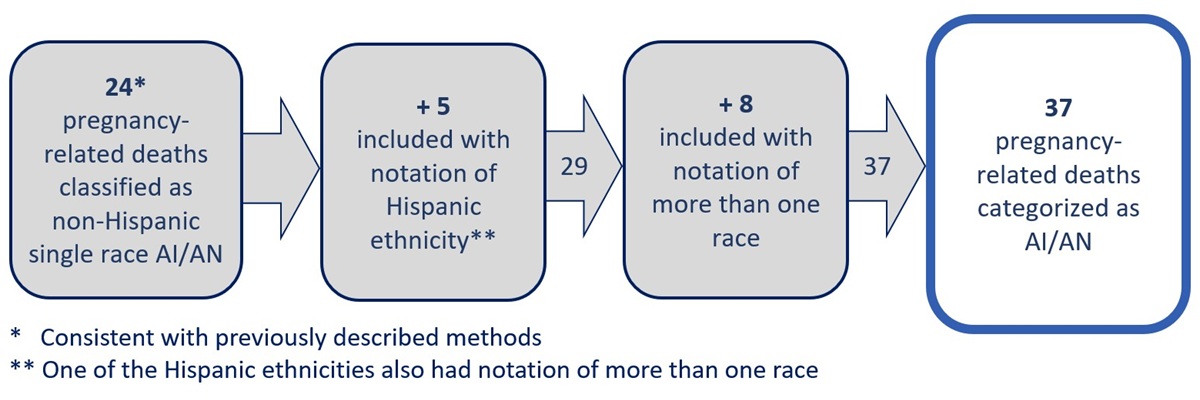
In the 2021 MMRIA data, 24 pregnancy-related deaths were classified as non-Hispanic single-race AI/AN. As shown in Figure 3, by using an alternate approach to classifying available vital records information on race and ethnicity, 37 pregnancy-related deaths were classified as AI/AN.
Because of known limitations of vital records data for identifying AI/AN women4, 37 is still likely an undercount of deaths among AI/AN women.
Figure 3. Classification of pregnancy-related deaths among American Indian or Alaska Native in Data from MMRCs in 46 US States, 2021
Data interpretation
- These data describe the distribution of characteristics among pregnancy-related deaths, but do not describe the estimated risk or disproportionate burden of pregnancy-related deaths by characteristics.
What the data include
CDC used race and ethnicity data from the birth or fetal death records, when available, and from death records when a birth record or fetal death record was unavailable. Race and Hispanic origin are reported separately on the birth, fetal, and death records; more than one race can be selected. CDC combined race and ethnicity information into a single categorical variable. All deaths with a notation of American Indian or Alaska Native are classified as American Indian or Alaska Native. The remaining deaths with a notation of Hispanic origin are classified as Hispanic. For deaths with missing notation of Hispanic origin, race-ethnicity of the decedent was classified as missing. For deaths with a notation of non-Hispanic origin but a notation that race was missing, the race-ethnicity of the decedent was classified as missing. For non-Hispanic women, race was classified as: non-Hispanic single-race White, non-Hispanic single-race Black, non-Hispanic single-race American Indian or Alaska Native (AI/AN), non-Hispanic single-race Asian, non-Hispanic single-race Native Hawaiian or Other Pacific Islander (NHOPI). For brevity, text and tables omit the term single-race. Free text from the "Other Race" field was not used for 2017-2019 and 2020 data but was used for the 2021 data. When Other race or more than one race were noted, race was classified as non-Hispanic other/multiple races.
CDC used age information from the death record.
CDC used education level from the birth or fetal death record, when available, and from death records when a birth or fetal death record was unavailable, with one exception. For the 2017 - 2019 data, if the death occurred during the postpartum period, and the death record indicated an education one level higher than the birth record, we relied on the higher education level from the death record.
Geographic information is based on county of last residence from the death record, when available, and from the birth or fetal death record when missing or undetermined on the death record. Geographic classifications are those produced by Texas A&M Geoservices.
Urban classification includes metropolitan division (≥2,500,000) and metropolitan (≥50,000-2,499,999). Rural classification includes micropolitan (10,000-49,999) and rural (<10,000) as captured in MMRIA.
Timing of death in relation to pregnancy was assigned by using the number of days between the date of death and the end of pregnancy, as documented by the MMRC abstractor, or as calculated by using the number of days between the date of death on the death record and the date of birth or fetal death on the linked birth or fetal death record by CDC. Deaths classified as occurring on the "day of delivery" occurred within 24 hours of the end of pregnancy. If timing of death was missing, deaths with the standard pregnancy checkbox on the death certificate marked as "Pregnant at the time of death" were classified as "during pregnancy." When available, the timing of death documented in the narrative was used to classify timing of deaths when deaths were missing a timing classification based on the number of days, abstractor-assigned category, and pregnancy checkbox. Deaths that did not have enough information to determine the exact timing of death and where a narrative was available were classified as unknown, while deaths without a narrative were classified as missing.
Data definitions
Pregnancy-Related
A death during pregnancy or within one year of the end of pregnancy from a pregnancy complication, a chain of events initiated by pregnancy, or the aggravation of an unrelated condition by the effects of pregnancy. In addition to having a temporal relationship to pregnancy, these deaths are causally related to pregnancy or its management.
Preventability
A death is considered preventable if the committee determines that there was at least some chance of the death being averted by one or more reasonable changes to patient, community, provider, facility, and/or systems factors. MMRIA allows MMRCs to document preventability decisions in two ways: (1) determining preventability as a yes or no, and/or 2) determining the chance to alter the outcome by using a scale that indicates no chance, some chance, or good chance. Any death with a yes response or a response that there was some chance or a good chance to alter the outcome was considered preventable. Deaths with a no response or no chance were considered not preventable.
There are four "circumstances surrounding a pregnancy-related death" that can be documented by MMRCs using standard checkboxes. The MMRC determination for a circumstance surrounding a pregnancy-related death documents if one of these circumstances both was present and contributed to the chain of events leading to a death but may not have been the underlying cause of death. The MMRC separately considers and documents each circumstance so each pregnancy-related death may have multiple circumstances identified. The options that a MMRC documents for each circumstance include: Yes, No, Probably, or Unknown.
The four circumstances are listed below.
Obesity
MMRCs determine whether obesity contributed to the death, and not just whether the woman was obese. The committee may determine that obesity contributed to the death when the condition directly compromised a women's health or health care. For example, obesity complicated ventilation options for a pregnant woman with the flu.
Discrimination
MMRCs determine whether discrimination contributed to the death, and not just whether the woman was exposed to discrimination. Discrimination is defined as treating someone less or more favorably based on the group, class, or category they belong to. For example, dismissing symptoms of abdominal pain described by a woman with a history of substance use disorder, which led to a delay in diagnosis and care for ruptured ectopic pregnancy. This determination was added as an option for MMRCs in MMRIA in May 2020.
Mental health conditions (other than substance use disorder)
MMRCs determine whether a mental health condition other than substance use disorder contributed to the death, and not just whether the woman had a mental health condition. Mental health conditions are defined as present when the woman had a documented diagnosis of a psychiatric disorder. This includes depressive, anxiety, psychotic, and bipolar disorders. If a documented diagnosis is not available, the committee will consult with their review committee subject matter experts (for instance, psychiatrist, psychologist, licensed counselor) to determine whether the criteria for a diagnosis of a mental health condition are met. The committee may determine that a mental health condition is a circumstance that contributed to the death when the condition directly compromised a women's health or health care (for example, mental health condition impacted her ability to manage type 2 diabetes).
Substance use disorder
MMRCs determine whether substance use disorder contributed to the death, and not just whether the woman had a substance use disorder. Substance use disorder is characterized by recurrent use of alcohol and/or drugs causing clinically and functionally significant impairment (for example, health problems or disability). Substance use disorder is documented separately from other mental health conditions as a circumstance surrounding a death. The committee may determine that substance use disorder is a circumstance that contributed to the death when the disorder directly compromised a women's health or health care (for instance, acute methamphetamine intoxication made preeclampsia worse, or she was more vulnerable to infections or medical conditions).
If a death is determined to be preventable, the MMRCs describe, using free text, contributing factors and recommendations among pregnancy-related deaths. For each contributing factor described, MMRCs select a contributing factor class from a standardized list of 27 specific contributing factor classes. Each preventable pregnancy-related death can have multiple contributing factors and classes. Below are details for select contributing factor classes.
Lack of Access/Financial Resources
Systemic barriers, e.g., lack or loss of healthcare insurance or other financial duress, as opposed to noncompliance, impacted their ability to care for themself (e.g., did not seek services because unable to miss work or afford postpartum visits after insurance expired). Other barriers to accessing care: insurance non-eligibility, provider shortage in their geographical area, and lack of public transportation.
Chronic Disease
Occurrence of one or more significant pre-existing medical conditions (e.g., obesity, cardiovascular disease, or diabetes).
Clinical Skill/Quality of Care
Personnel were not appropriately skilled for the situation or did not exercise clinical judgment consistent with standards of care (e.g., error in the preparation or administration of medication or unavailability of translation services).
Knowledge-Lack of knowledge regarding importance of event or of treatment or follow-up
The provider or patient did not receive adequate education or lacked knowledge or understanding regarding the significance of a health event (e.g., shortness of breath as a trigger to seek immediate care) or lacked understanding about the need for treatment/follow-up after evaluation for a health event (e.g., needed to keep appointment for psychiatric referral after an ED visit for exacerbation of depression).
Lack of continuity of care (provider or facility perspective)
Care providers did not have access to woman's complete records or did not communicate their status sufficiently. Lack of continuity can be between prenatal, labor and delivery, and postpartum providers.
Substance use disorder – alcohol, illicit/prescription drugs
Substance use disorder is characterized by recurrent use of alcohol and/or drugs causing clinically and functionally significant impairment, such as health problems or disability. The committee may determine that substance use disorder contributed to the death when the disorder directly compromised their health status (e.g., acute methamphetamine intoxication exacerbated pregnancy- induced hypertension, or they were more vulnerable to infections or medical conditions).
Failure to screen/inadequate assessment of risk
Factors placing the woman at risk for a poor clinical outcome recognized, and they were not transferred/transported to a provider able to give a higher level of care.
Delay
The provider or patient was delayed in referring or accessing care, treatment, or follow-up care/action.
Discrimination
Treating someone less or more favorably based on the group, class or category they belong to.
MMRCs select one of five class levels for each identified contributing factor class (i.e., where the factor manifested): patient/family, provider, facility, system, and community.
MMRCs also select one of five class levels for each prevention recommendation (i.e., where the prevention recommendation should be applied): patient/family, provider, facility, system, and community.
The levels are described below.
Patient/Family
A woman before, during or after a pregnancy, and her family, internal or external to the household, with influence on the woman
Provider
An individual with training and expertise who provides care, treatment, and/or advice
Facility
A physical location where direct care is provided - ranges from small clinics and urgent care centers to hospitals with trauma centers
System
Interacting entities that support services before, during, or after a pregnancy - ranges from healthcare systems and payors to public services and programs
Community
A grouping based on a shared sense of place or identity - ranges from physical neighborhoods to a community based on common interests and shared circumstances.
The underlying cause of death refers to the disease or injury that initiated the chain of events leading to death or the circumstances of the accident or violence that produced the fatal injury. MMRCs determine the underlying cause of death and assign a PMSS-MM code for each pregnancy-related death. These codes are grouped into categories.
Below are details for select underlying cause of death categories.
Mental Health Conditions
Mental health conditions include deaths to suicide, unintentional or unknown intent overdose/poisoning related to substance use disorder, and other deaths determined by the MMRC to be related to a mental health condition, including substance use disorder.
During analysis some deaths that were either missing a MMRC determined cause of death code or that had an injury cause of death code were included in the metal health condition category: 1) Suicide deaths are those deaths with an MMRC response of 'yes' or 'probably' for the question 'was this death a suicide?'. 2) Deaths that the MMRCs determined the means of fatal injury to be poisoning/overdose and substance use disorder contributed to the death and Unintentional or unknown intent poisoning/overdose deaths are defined as deaths with an MMRC response of missing, 'unknown' or 'no' for the question 'was this death a suicide?' Deaths with an MMRC response of missing, 'unknown', 'not applicable', or 'other' for the means of fatal injury field and with a death record or autopsy cause of death indicating an overdose (i.e., acute toxicity, acute intoxication, multiple drug intoxication, overdose) were assigned as unintentional or unknown intent poisoning/overdose deaths.
Cardiovascular Conditions
Cardiomyopathy, and coronary artery disease, pulmonary hypertension, acquired and congenital valvular heart disease, vascular aneurysm, hypertensive cardiovascular disease, Marfan Syndrome, conduction defects, vascular malformations, and cardiovascular disease not otherwise specified (NOS); excludes cerebrovascular accident (CVA) and hypertensive disorders of pregnancy.
Beginning in 2020, a new category for grouping Cardiovascular conditions was introduced. This Cardiovascular condition category includes deaths with underlying causes of cardiomyopathy and other cardiovascular conditions. Other cardiovascular conditions were referred to as cardiac and coronary condition in previous reports.
Infection
Infection includes postpartum genital tract infection, sepsis/septic shock, chorioamnionitis/antepartum infection, urinary tract infection, influenza, COVID-19, pneumonia, other non-pelvic infection, and other infection not otherwise specified (NOS). Beginning in 2020, COVID-19 could be documented by MMRCs as an underlying cause of death and is included in the infection category.
- Improving Data Capacity for American Indian/Alaska Native (AI/AN) Populations in Federal Health Surveys. HHS Office of the Assistant Secretary for Planning and Evaluation; 2019.
- Best Practices for American Indian and Alaska Native Data Collection. Seattle, WA: Urban Indian Health Institute; 2020.
- Joshi S, Warren-Mears V. Identification of American Indians and Alaska Natives in Public Health Data Sets: A Comparison Using Linkage-Corrected Washington State Death Certificates. J Public Health Manag Pract. 2019 Sep/Oct;25 Suppl 5, Tribal Epidemiology Centers: Advancing Public Health in Indian Country for Over 20 Years:S48-S53.
- Anderson RN, Copeland G, Hayes JM. Linkages to improve mortality data for American Indians and Alaska Natives: a new model for death reporting? Am J Public Health. 2014 Jun;104 Suppl 3(Suppl 3):S258-62.
- Trost SL, Beauregard J, Njie F, et al. Pregnancy-Related Deaths: Data from Maternal Mortality Review Committees in 36 US States, 2017-2019. Atlanta, GA: Centers for Disease Control and Prevention, US Department of Health and Human Services; 2022.
- Hardeman RR, et al. Developing Tools to Report Racism in Maternal Health for the CDC Maternal Mortality Review Information Application (MMRIA): Findings from the MMRIA Racism & Discrimination Working Group. Matern Child Health J. 2022 Apr;26(4):661-669.