Key points
This chapter provides general guidance for vaccine-preventable disease surveillance, describing the disease background/epidemiology, case investigation and reporting/notification, disease case definitions, and activities for enhancing surveillance, case investigation, and outbreak control for pneumococcal.
Disease Description
Streptococcus pneumoniae (pneumococcus) is a gram-positive bacterium with more than 100 known serotypes. Pneumococcus is spread by airborne droplets and is a leading cause of serious illness, including sepsis, meningitis, and pneumonia among children and adults worldwide.12 Although all serotypes can cause serious disease, a relatively limited number of serotypes cause the majority of invasive pneumococcal disease (IPD).
The Centers for Disease Control and Prevention's (CDC's) Active Bacterial Core Surveillance (ABCs) has tracked IPD in selected regions of the United States since 1995.3 ABCs data indicate that younger children and older adults have the highest rates of invasive disease (Table 1).24 Approximately 10% of all patients with IPD die of their illness, but case-fatality rates are higher for older adults and patients with certain underlying illnesses.45
Table 1. Incidence of Invasive pneumococcal disease at ABCs sites in the United States, 20224
| Age (years) | Disease Incidence Cases/100,000 | Death Rate Deaths/100,000 |
|---|---|---|
| <1 | 10.8 | 0.5 |
| 1 | 7.6 | 0.0 |
| 2−4 | 6.8 | 0.3 |
| 5−17 | 2.3 | 0.1 |
| 18−34 | 3.1 | 0.2 |
| 35−49 | 7.4 | 0.6 |
| 50−64 | 13.2 | 1.8 |
| 65−74 | 15.8 | 1.7 |
| 75−84 | 16.4 | 2.7 |
| ≥85 | 27.4 | 7.5 |
| Total | 8.3 | 1.0 |
Each year in the United States, pneumococcal disease accounts for a substantial number of cases of invasive and non-invasive disease including meningitis, sepsis, pneumonia, sinusitis, and acute otitis media (AOM).456789 Prior to the COVID-19 pandemic, approximately 30,000 IPD cases 3,000 deaths from IPD occurred each year in the United States.4Estimating the number of non-invasive pneumococcal disease cases remains challenging due to limitations with diagnostic testing. Recent estimates suggest more than 2 million pneumococcal infections occur annually, resulting in 6,000 deaths.10
Pneumococcal disease is preceded by asymptomatic colonization of the nasopharynx which tends to be especially common in children.11 AOM is the most common clinical manifestation of pneumococcal infection among children and the most common outpatient diagnosis resulting in antibiotic prescriptions in that group.12 In adults, pneumonia is the most common clinical manifestation, causing an estimated 150,000 hospitalizations each year in the United States.10
Background
Trends in invasive pneumococcal disease
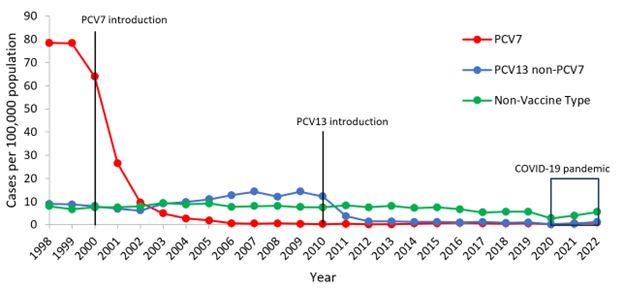
A 7-valent pneumococcal conjugate vaccine (PCV7) was introduced in U.S. children aged <5 years in 2000. Following the introduction of PCV7, dramatic declines in IPD were reported among children aged <5 years. Rates of IPD caused by the 7 serotypes included in the vaccine declined from around 80 cases per 100,000 population in 1998-1999, to less than 1 case per 100,000 population by 2007 (Figure 1).13
Figure 1. Rates of invasive pneumococcal disease among children <5 years of age, 1998–20224
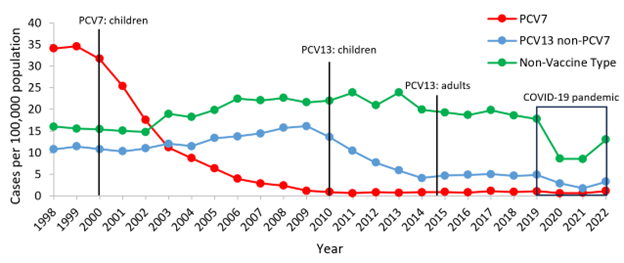
The use of PCV7 in children aged <5 years also reduced the burden of IPD among older children and adults through reduced transmission of vaccine serotype pneumococci (herd protection). In 1998-99, rates of PCV7-type IPD among adults aged ≥65 years were around 40 cases per 100,000 population. After the introduction of PCV7, rates of disease due to these 7 serotypes had declined 45% by 2007 (Figure 2).1314151617
Figure 2. Rates of invasive pneumococcal disease among U.S. adults >65 years of age, 1998–2022 4
At the same time, increases in disease caused by serotypes not included in PCV7 (i.e., non-vaccine serotypes or NVT) were observed among children and adult populations, although these increases were small in magnitude compared with the overall reduction in disease.131415161718 An increase in disease caused by non-vaccine serotypes after vaccine introduction is called replacement disease.
In 2010, a new 13-valent conjugate vaccine (PCV13) was introduced in children aged <5 years. This vaccine included the original 7 serotypes in PCV7 plus 6 additional serotypes (Table 2). After the introduction of PCV13, cases of invasive disease due to the six additional serotypes covered by the vaccine (PCV13 non-PCV7) declined substantially.17 In 2007-08 (pre-PCV13), rates of PCV13-type IPD among children aged <5 years were around 14 cases per 100,000 population. In 2014-15 (post-PCV13), rates of PCV13-type disease had decreased by 87%. Declines plateaued after 2015 and remained stable through 2019 (Figure 1).4
After introduction of PCV13 in children, older adults also saw reductions in IPD through herd protection. In 2007-08, rates of PCV13-type IPD among adults aged ≥65 years were around 17 cases per 100,000 population. In 2014-15, rates of PCV13-type disease had decreased by 70% (Figure 2). No significant increases in non-PCV13-type IPD have been observed in any age group since the introduction of PCV13. In late 2014, PCV13 was approved for routine use among adults aged ≥65 years. No additional declines in PCV13-type IPD were observed in adults aged ≥65 years after introduction of PCV13 in 2014. In 2020, during the COVID-19 pandemic, rates of IPD declined sharply in all age groups.19 However, in 2021–2022 rates of IPD rebounded in both children and adults (Figures 1&2).
New higher valency PCVs (PCV15, PCV20) were recommended for adults in 2021.20 PCV15 and PCV20 were also recommended for children in 2022 and 2023, respectively.2122 Additionally, in 2024, PCV21 was recommended for adults.23 With the impact of the recent COVID-19 pandemic and rapid introduction of several new vaccines in both children and adults, it is vital to continue monitoring IPD trends in the U.S. to determine the impact of these new vaccines. Up-to-date trends for U.S. IPD cases can be found on ABCs Bact Facts Interactive Data Dashboard.
Antimicrobial resistance trends
Before 1990, S. pneumoniae was almost uniformly susceptible to penicillin, allowing most clinicians to treat persons with severe infections with penicillin alone. However, during the 1990's, resistance to penicillin and to multiple classes of antibiotics spread rapidly in the United States with an increasing trend of invasive pneumococci resistant to three or more antibiotic classes (defined as S. pneumoniae isolates that are either intermediate or fully resistant to three antibiotics tested).24252627 As of 2018, CDC estimated there were 900,000 infections and 3,600 deaths associated with drug-resistant Streptococcus pneumoniae (DRSP) infections.10 Up-to-date estimates of the burden of DRSP are published as part of CDC's Antibiotic Resistance Threats Report.
Following the introduction of PCV7 into the routine childhood immunization program in 2000, the incidence of antibiotic-resistant invasive disease declined substantially among both young children and older persons due to reductions in resistant infections caused by vaccine serotypes.1628293031 Between 1998–99 and 2008, penicillin-resistant IPD rates declined 64% for children aged <5 years of age and 45% for adults aged ≥65 years.31 An increase in penicillin-resistant disease caused by serotypes not included in PCV7 was also identified during the same time period, although the magnitude of this effect remained small.28 PCVs are not expected to reduce the incidence of DRSP caused by non-vaccine type (NVT) serotypes. The prevalence of antibiotic resistance varied by geographic area both before and after PCV7 introduction, with higher prevalence noted in the southeastern United States.2425262728
During 2007–08, PCV13 non-PCV7 serotypes caused 78–97% of penicillin-resistant IPD, depending on age.31 Serotype 19A, a PCV13 non-PCV7 serotype, accounted for more than 30% of DRSP during 2005–2009 prior to PCV13 introduction.32 The introduction of PCV13 in 2010 led to further reductions in antibiotic-resistant IPD rates, particularly among serotype 19A. From 2009-2013 rates of antibiotic-resistant IPD caused by PCV13 non-PCV7 serotypes decreased by 97% among children aged <5 years, and 64% among adults aged ≥65 years.33 In 2008, the Clinical and Laboratory Standards Institute (CLSI) established new, higher minimum inhibitory concentration (MIC) breakpoints for defining pneumococcal susceptibility to parenterally administered penicillin when treating pneumococcal disease other than meningitis.34 Regardless of whether the old or new parenteral penicillin breakpoints are used, penicillin-resistant IPD caused by PCV13 serotypes has decreased substantially for all age groups.3133 However, during this period, rates of antibiotic-resistant IPD due to non-PCV13-type increased in all age groups.
Introduction of higher valency PCVs that contain additional pneumococcal serotypes (PCV15, PCV20, PCV21) is expected to further reduce the incidence of antibiotic resistant IPD. During 2014-2018, additional serotypes included in PCV15 and PCV20 (but not included in PCV13) contributed to 19% and 24% of all antibiotic-resistant IPD cases, respectively.32 Introduction of these higher valency vaccines is expected to further avert antibiotic use for outpatient bacterial respiratory infections and therefore the burden of DRSP.35
Because of a lack of rapid, sensitive, and specific diagnostic tests, acute respiratory tract infections treated in outpatient settings remains empiric. Inappropriate antibiotic use contributes to the development of DRSP. Principles have been developed to avoid unnecessary antibiotic use and emphasize appropriate selection and duration of antibiotic therapy when indicated for adults and children with upper respiratory infections.36373839 Groups of experts have provided national guidance for treating infections commonly caused by pneumococcus, such as AOM and pneumonia, considering emergence of DRSP.36373839
Importance of Surveillance
Surveillance for IPD has four main goals:
- Characterization of national and local trends of IPD,
- Detection of geographic and temporal changes in the prevalence of DRSP,
- Monitoring impact of vaccines on IPD, and
- Informing future vaccine development.
Surveillance for IPD in persons aged ≥5 years is useful to monitor the impact of the herd effects of pediatric PCV use and replacement disease. Following the introduction of new PCVs since 2021, monitoring disease trends in both children and adults is important to assess the impact of the updated vaccine recommendations.20212223
Serotyping of pneumococcal isolates can improve understanding of the vaccine impact. However, serotyping is expensive and requires specialized reagents and extensive technical training; therefore, serotyping capacity is not widely available. The use of polymerase chain reaction (PCR) or whole genome sequencing to identify pneumococcal capsular genes specific for individual capsular serotypes may be feasible for some state public health and academic research centers.4041 CDC's Streptococcus Laboratory has developed a protocol to identify pneumococcal serotypes using PCR.
Pneumococcal surveillance enables recognition of new or rare resistance patterns.42 Surveillance information can be used on the national level for research and policy development and at the state or local level to raise awareness of DRSP among healthcare providers and the general public. Surveillance data also may be useful for tracking the impact of interventions aimed at reducing unnecessary use of antimicrobial agents.
CDC's Antibiotic Resistance Laboratory Network (ARLN) program can assist state and local health departments with Clinical Laboratory Improvement Amendments (CLIA) approved serotyping and antimicrobial susceptibility testing for IPD isolates that meet certain criteria. For additional information on serotyping requests, contact ARLN@cdc.gov.
Disease Reduction Goals
Continuous surveillance is important to evaluate the impact of PCVs on the incidence of IPD, DRSP infections, and to monitor disease caused by pneumococcal serotypes not included in PCVs (i.e., replacement disease).
Disease reduction goals also focus on minimizing complications of DRSP infections through prevention and control measures. Geographic differences in antibiotic prescribing practices have been described.43 In sites where antibiotic prescribing is high, the proportion of IPD resistant to antibiotics is also high, suggesting that local prescribing practices may contribute to local resistance patterns.43
In 2003, CDC launched a national educational campaign now known as Be Antibiotics Aware: Smart Use, Best Care. The campaign provides resources to healthcare providers and the public about antibiotic resistance and how to optimize antibiotic prescribing and use. In 2014, CDC released the Core Elements of Antibiotic Stewardship to provide a set of key principles for healthcare facility leaders and healthcare providers to facilitate efforts to improve the quality of antibiotic use. The Core Elements framework has been adapted for several healthcare settings, including outpatient settings, and emphasizes the importance of appropriate management of respiratory infections.
Case Definition
Beginning in 2017, a new "probable" case classification was added to capture cases diagnosed using culture-independent diagnostic tests (CIDTs) and replaced the "suspected" case definition. The following definitions are in use for national notification of IPD in the United States.
Confirmed: Isolation of S. pneumoniae from a normally sterile site (e.g., blood, cerebrospinal fluid, or, less commonly, joint, pleural or pericardial fluid). (Event code 11723)
Probable: Identification of S. pneumoniae from a normally sterile body site by a CIDT without isolation of the bacteria.44
Confirmed and suspected cases of IPD should be reported to public health authorities within 1 week of diagnosis. CSTE also recommends certain clinical and epidemiological information be collected, including date of illness onset, clinical syndrome (e.g., pneumonia, meningitis), underlying medical conditions, type of diagnostic test used, and pneumococcal vaccination history. DRSP is no longer collected in national surveillance as a separate event from IPD.45
Laboratory Testing
Refer to Chapter 22: Laboratory Support for Surveillance of Vaccine-Preventable Diseases | Manual for the Surveillance of Vaccine-Preventable Diseases | CDC for detailed information on laboratory testing for IPD and for specific information on specimen collection and shipment.
Specimen collection
Specimen collection and shipping are important steps in obtaining laboratory diagnosis or disease confirmation. Guidelines have been published for specimen collection and handling for viral and microbiologic agents. Information is also available on using CDC laboratories as support for reference and disease surveillance; resources include:
- A central website for requesting lab testing
- The CDC Infectious Diseases Laboratory Specimen Submission Form
- Information on general requirements for shipment of etiologic agents (Appendix 24 [4 pages]) Similarly to CDC, state laboratories provide online test directories containing lists of orderable tests for that institution, along with appropriate specimen types, collection methods, specimen volume, and points of contact
Reporting and Case Notification
Case reporting within a jurisdiction
Each state and territory (jurisdiction) has regulations and laws governing the reporting of diseases and conditions of public health importance.46 These regulations and laws list the diseases that are to be reported, and describe those persons or institutions responsible for reporting, such as healthcare providers, hospitals, laboratories, schools, daycare and childcare facilities, and other institutions. Detailed information on reportable conditions in each jurisdiction is available through CSTE.47
Most jurisdictions currently require IPD to be reported to local or state/jurisdiction health authorities, regardless of the age of the patient or presence of drug resistance. Additional jurisdictions require reporting in limited populations, such as children <5 years of age. In jurisdictions with reporting requirements, confirmed and probable cases of IPD should be reported to state/jurisdiction or local health departments by healthcare providers, which may include clinicians, laboratories, hospitals, and pharmacies.4748 Healthcare providers should identify cases through microbiology laboratories, death certificates, hospital discharge or outpatient records, and electronic medical records. The following data are recommended for case investigation and reporting: patient's date of birth or age, the anatomic site of specimen collection, and type of infection. Other epidemiological information that is preferred includes the patient's demographic information (i.e., sex, race, and ethnicity), specimen collection date, whether the patient was hospitalized, clinical syndrome, antibiotic susceptibility, details of pneumococcal vaccination history, underlying medical conditions, outcome, and any serotyping results available (if an isolate was tested). Additional information may be collected at the direction of the state or local health department. The S. pneumoniae Surveillance Worksheet is included as Appendix 13 to serve as a guide for data collection during investigation of reported cases.
Case notification to CDC
Notifications for confirmed cases of IPD should be sent to CDC using event code 11723 in the National Notifiable Diseases Surveillance System (NNDSS).4549 The S. pneumoniae Surveillance Worksheet is included as Appendix 13, to serve as a guide for data collection to be included in case investigations and case notification to CDC. Case notification should not be delayed because of incomplete information or lack of confirmation. The jurisdiction in which the patient resides at the time of diagnosis should submit the case notification to CDC.
Vaccination
For specific information about pneumococcal vaccination, refer to the CDC website, which provides general recommendations, including vaccine use and scheduling, immunization strategies for providers, vaccine content, adverse events and reactions, vaccine storage and handling, and contraindications and precautions. A free mobile app is available to help determine patient-specific pneumococcal vaccine recommendations.
Enhancing Surveillance
Several surveillance activities may improve the detection and reporting of pneumococcal disease and the quality of the reports.
Enhancing reporting of antibiotic susceptibility results
Concern over rising resistance to antibiotics has prompted many state or local health departments to increase their focus on reporting susceptibility results. CDC has worked with jurisdiction health departments to evaluate different surveillance methods to determine which methods would enhance the reliability of surveillance data, given certain goals and resource limitations.50 Use of aggregated antibiogram data collected from all hospital laboratories within a specific area has been shown to give a relatively accurate description of the proportion of isolates that are resistant to penicillin and a limited number of other drugs.51 Such data, however, typically cannot be analyzed by age group or other factors of interest. Sentinel systems, which may collect individual reports with more details from a limited number of laboratories, can give an accurate view of resistance if designed well.52
Encouraging provider reporting
Most jurisdictions' infectious disease surveillance systems depend upon the receipt of case reports from healthcare providers and laboratories. These data are often incomplete and may not be representative of certain populations.46 It is important for healthcare providers to understand which events should be reported, and how critical accurate reporting is for control of communicable diseases. Increasing provider awareness of local rates of IPD and local reporting requirements may enhance surveillance.
Improving detection of DRSP in laboratories
Universal adoption of optimal testing methods and testing for resistance to recommended antibiotics would improve our ability to detect and monitor resistant pathogens.34
Recommended antibiotics to test for include53
- Erythromycin
- Penicillin
- Trimethoprim-sulfamethoxazole
- Cefotaxime
- Ceftriaxone
- Meropenem
- Clindamycin
- Doxycycline
- Tetracycline
- Levofloxacin
- Moxifloxacin
- Vancomycin
Streamlining reporting using electronic methods
Use of data from sources such as electronic medical records, electronic case reporting, and laboratory information management systems can significantly improve reporting speed, enhance data quality, and reduce workload.
Case Investigation
As with many respiratory pathogens, rapid, sensitive, and specific diagnostic tests are not widely available for pneumococcal disease. An assay to detect pneumococcal antigen in urine can be used to rapidly diagnose pneumococcal pneumonia and invasive pneumococcal disease like meningitis in adults. In addition, a multiplex PCR diagnostic test that detects S. pneumoniae in lower respiratory specimens is now available. Regardless, early in the course of illnesses such as pneumonia, diagnosis of S. pneumoniae infection is often presumptive and the choice of antimicrobial therapy is nearly always empiric. However, once S. pneumoniae is isolated from a normally sterile body site, antibiotic susceptibility testing results could help guide patient management. Case investigations are not usually warranted, except in outbreaks or as determined by the state health department. CDC is available during outbreaks to assist with epidemiologic and laboratory investigations. Contact pneumococcus@cdc.gov for additional information.
Authors and Suggested Citation
Ryan Gierke, MPH; Sopio Chochua, PhD, Kristin Andrejko, PhD; Lesley McGee, PhD; Miwako Kobayashi, MD, MPH
Suggested citation:
Given the variations in the timing for when chapter updates are made, a Manual edition number is no longer used. Therefore, it is recommended that the date at the top right of the web page be used in references/citations.
Content source:
National Center for Immunization and Respiratory Diseases
- Nuorti JP, Whitney CG, Centers for Disease Control and Prevention. Prevention of pneumococcal disease among infants and children — use of 13-valent pneumococcal conjugate vaccine and 23-valent pneumococcal polysaccharide vaccine: Recommendations of the Advisory Committee on Immunization Practices (ACIP).MMWR Recomm Rep. 2010;59(RR-11):1–18.
- Thigpen MC, Whitney CG, Messonnier NE, et al. Bacterial meningitis in the United States, 1998–2007. N Engl J Med. 2011;364(21):2016–25. doi:10.1056/NEJMoa1005384
- Schuchat A, Hilger T, Zell E, et al. Active Bacterial Core surveillance of the Emerging Infections Program Network. Emerg Infect Dis. 2001;7(1):92–9. doi: 10.3201/eid0707.017711
- CDC. Bact Facts Interactive. Active Bacterial Core surveillance (ABCs). May 28, 2024. Accessed October 28, 2024.
- Robinson KA, Baughman W, Rothrock G, et al. Epidemiology of invasive Streptococcus pneumoniae infections in the United States, 1995–1998: Opportunities for prevention in the conjugate vaccine era.Jama. 2001;285(13):1729–35. doi: 10.1001/jama.285.13.1729
- Centers for Disease Control and Prevention. Prevention of pneumococcal disease: Recommendations of the Advisory Committee on Immunization Practices (ACIP).MMWR Recomm Rep. 1997;46(RR-8):1–24.
- Dowell SF, Marcy SM, Phillips WR, Gerber MA, Schwartz B. Otitis media—Principles of judicious use of antimicrobial agents.Pediatrics. 1998;101:165–71. https://doi.org/10.1542/peds.101.S1.165
- Block SL, Hedrick J, Harrison CJ, et al. Community-wide vaccination with the heptavalent pneumococcal conjugate significantly alters the microbiology of acute otitis media. Pediatr Infect J. 2004;23(9):829–33. doi: 10.1097/01.inf.0000136868.91756.80
- Casey JR, Pichichero ME. Changes in frequency and pathogens causing acute otitis media in 19952003.Pediatr Infect J. 2004;23(9):824–8. doi: 10.1097/01.inf.0000136871.51792.19
- CDC. 2019 Antibiotic resistance threats report. Antimicrobial resistance. July 17, 2024. Accessed October 28, 2024.
- Bogaert D, De Groot R, Hermans PW. Streptococcus pneumoniae colonisation: The key to pneumococcal disease.Lancet Infect Dis. 2004;4(3):144–54. doi:10.1016/S1473-3099(04)00938-7
- Centers for Disease Control and Prevention. Preventing pneumococcal disease among infants and young children: Recommendations of the Advisory Committee on Immunization Practices (ACIP).MMWR. 2000;49(No. RR-9):1–35.
- Pilishvili T, Lexau C, Farley MM, et al. Sustained reductions in invasive pneumococcal disease in the erf conjugate vaccine.J Infect Dis. 2010;201(1):32–41. doi:10.1086/648593
- Lexau CA, Lynfield R, Danila R, et al. Changing epidemiology of invasive pneumococcal disease among older adults in the era of pediatric pneumococcal conjugate vaccine.Jama. 2005;294(16):2043–51.
- Moore MR, Pilishvili T, Bennett N, et al. Trends in invasive pneumococcal disease among adults, 1998-2004: Implications for conjugate vaccine development. International Conference on Emerging Infectious Diseases. 2006; Atlanta, GA; 2006.
- Whitney CG, Farley MM, Hadler J, et al. Decline in invasive pneumococcal disease after the introduction of protein-polysaccharide conjugate vaccine.N Engl J Med. 2003;348(18):1737–46. doi:10.1056/NEJMoa022823
- Moore MR, Link-Gelles R, Schaffner W, et al. Impact of use of 13-valent pneumococcal conjugate vaccine in children on invasive pneumococcal disease in children and adults in the USA: Analysis of multisite, population-based surveillance.Lancet Infect Dis. 2015;15(3):301–9. doi:10.1016/s1473-3099(14)71081-3
- Centers for Disease Control and Prevention. Direct and indirect effects of routine vaccination of children with 7-valent pneumococcal conjugate vaccine on incidence of invasive pneumococcal disease—United States, 1998–2003.MMWR Morb Mortal Wkly Rep. 2005;54(36):893–7.
- Prasad N, Rhodes J, Deng L, et al. Changes in the incidence of invasive bacterial disease during the COVID-19 pandemic in the United States, 2014–2020. J Infect Dis. 2023;227(7):907–916. doi:10.1093/infdis/jiad028
- Kobayashi M, Farrar JL, Gierke R, et al. Use of 15-valent pneumococcal conjugate vaccine and 20-valent pneumococcal conjugate vaccine among U.S. adults: updated recommendations of the Advisory Committee on Immunization Practices — United States, 2022. MMWR Morb Mortal Wkly Rep. 2022;71(4):109–17. doi:10.15585/mmwr.mm7104a1v
- Kobayashi M, Farrar JL, Gierke R, et al. Use of 15-valent pneumococcal conjugate vaccine among U.S. children: Updated recommendations of the Advisory Committee on Immunization Practices —United States, 2022.MMWR Morb Mortal Wkly Rep. 2022;71(37):1174–81. doi:10.15585/mmwr.mm7137a3
- CDC MMWR. ACIP updates: recommendations for use of 20-valent pneumococcal conjugate vaccine in children ― United States, 2023.MMWR Morb Mortal Wkly Rep. 2023;72. doi:10.15585/mmwr.mm7239a5
- Kobayashi M. Use of 21-valent pneumococcal conjugate vaccine among U.S. adults: recommendations of the Advisory Committee on Immunization Practices — United States, 2024.MMWR Morb Mortal Wkly Rep. 2024;73. doi:10.15585/mmwr.mm7336a3
- Whitney CG, Farley MM, Hadler J, et al. Increasing prevalence of multidrug-resistant Streptococcus pneumoniae in the United States.N Engl J Med. 2000;343(26):1917–24.
- Pletz MW, McGee L, Jorgensen J, et al. Levofloxacin-resistant invasive Streptococcus pneumoniae in the United States: Evidence for clonal spread and the impact of conjugate pneumococcal vaccine.Antimicrob Agents Chemother. 2004;48(9):3491–7.
- Butler JC, Hofmann J, Cetron MS, Elliott JA, Facklam RR, Breiman RF. The continued emergence of drug-resistant Streptococcus pneumoniae in the United States: An update from the Centers for Disease Control and Prevention's Pneumococcal Sentinel Surveillance System.J Infect Dis. 1996;174(5):986–93.
- Breiman RF, Butler JC, Tenover FC, Elliott JA, Facklam RR. Emergence of drug-resistant pneumococcal infections in the United States.Jama. 1994;271(23):1831–5.
- Kyaw MH, Lynfield R, Schaffner W, et al. Effect of introduction of the pneumococcal conjugate vaccine on drug-resistant Streptococcus pneumoniae.N Engl J Med. 2006;354(14):1455–63.
- Kaplan SL, Mason EO, Wald ER, et al. Decrease of invasive pneumococcal infections in children among 8 children's hospitals in the United States after the introduction of the 7-valent pneumococcal conjugate vaccine.Pediatrics. 2004;113(3 Pt 1):443–9.
- Stephens DS, Zughaier SM, Whitney CG, et al. Incidence of macrolide resistance in Streptococcus pneumoniae after introduction of the pneumococcal conjugate vaccine: Population-based assessment.Lancet. 2005;365(9462):855–63. doi: 10.1016/S0140-6736(05)71043-6
- Hampton LM, Farley MM, Schaffner W, et al. Prevention of antibiotic-nonsusceptible Streptococcus pneumoniae with conjugate vaccines.J Infect Dis. 2012;205(3):401–11. doi:10.1093/infdis/jir755
- Bajema KL, Gierke R, Farley MM, et al. Impact of pneumococcal conjugate vaccines on antibiotic-nonsusceptible invasive pneumococcal disease in the United States.J Infect Dis. 2022;226(2):342–51. doi:10.1093/infdis/jiac154
- Tomczyk S, Lynfield R, Schaffner W, et al. Prevention of antibiotic-nonsusceptible invasive pneumococcal disease with the 13-valent pneumococcal conjugate vaccine.Clin Infect Dis Off Publ Infect Dis Soc Am. 2016;62(9):1119–25. doi:10.1093/cid/ciw067
- Clinical and Laboratory Standards Institute. Clinical and Laboratory Standards Institute. Performance standards for antimicrobial susceptibility testing; twenty-first informational supplement. In: CLSI Document-M100-S21. Vol 30. Clinical and Laboratory Standards Institute; 2011.
- King LM, Andrejko KL, Kabbani S, et al. Outpatient visits and antibiotic use due to higher-valency pneumococcal vaccine serotypes.J Infect Dis. 2024;230(4):821–31. doi:10.1093/infdis/jiae142
- Metlay JP, Waterer GW, Long AC, et al. Diagnosis and treatment of adults with community-acquired pneumonia. An official clinical practice guideline of the American Thoracic Society and Infectious Diseases Society of America.Am J Respir Crit Care Med. 2019;200(7):e45–e67. doi:10.1164/rccm.201908-1581S
- Smith DK, Kuckel DP, Recidoro AM. Community-acquired pneumonia in children: Rapid evidence review. Accessed December 17, 2024.
- Lieberthal AS, Carroll AE, Chonmaitree T, et al. The diagnosis and management of acute otitis media.Pediatrics. 2013;131(3):e964–e999. doi:10.1542/peds.2012-3488
- CDC. Clinical care of outpatient adult and pediatric populations. Antibiotic prescribing and use. May 9, 2024. Accessed December 16, 2024.
- Velusamy S, Tran T, Mongkolrattanothai T, Walker H, McGee L, Beall B. Expanded sequential quadriplex real-time polymerase chain reaction (PCR) for identifying pneumococcal serotypes, penicillin susceptibility, and resistance markers.Diagn Microbiol Infect Dis. 2020;97(2):115037. doi:10.1016/j.diagmicrobio.2020.115037
- Metcalf BJ, Gertz RE, Gladstone RA, et al. Strain features and distributions in pneumococci from children with invasive disease before and after 13-valent conjugate vaccine implementation in the USA.Clin Microbiol Infect. 2016;22(1):60.e9–60.e29. doi:10.1016/j.cmi.2015.08.027
- Chochua S, Beall B, Lin W, et al. The emergent invasive serotype 4 ST10172 strain acquires vanG type vancomycin-resistance element: a case of a 66-year-old with bacteremic pneumococcal pneumonia.J Infect Dis. 2024 Aug 8:jiae393. Online ahead of print. doi:10.1093/infdis/jiae393
- Hicks LA, Chien YW, Taylor TH, Haber M, Klugman KP. Outpatient antibiotic prescribing and nonsusceptible Streptococcus pneumoniae in the United States, 1996–2003.Clin Infect Dis. 2011;53(7):631–9. doi:10.1093/cid/cir443
- CDC. Invasive pneumococcal disease (IPD) (Streptococcus pneumoniae) 2017 case definition | CDC. August 12, 2022. Accessed December 17, 2024.
- Council of State and Territorial Epidemiologists. Enhancing state-based surveillance for invasive pneumococcal disease. Published online 2009.
- Roush S, Birkhead G, Koo D, Cobb A, Fleming D. Mandatory reporting of diseases and conditions by health care professionals and laboratories.Jama. 1999;282(2):164–70.
- CSTE. STATE REPORTABLE CONDITIONS ASSESSMENT (SRCA) Council of State and Territorial Epidemiologists. Accessed December 17, 2024.
- Jajosky R, Rey A, Park M, Aranas A, Macdonald S, Ferland L. Findings from the Council of State and Territorial Epidemiologists' 2008 assessment of state reportable and nationally notifiable conditions in the United States and considerations for the future.J Public Health Manag Pract JPHMP. 2011;17(3):255–64. doi:10.1097/phh.0b013e318200f8da
- CDC. Event codes & other surveillance resources. April 5, 2024. Accessed December 17, 2024.
- Noggle B, Iwamoto M, Chiller T, Klevens M, Moore MR, Wright J, et al. Tracking resistant organisms: Workshop for improving state-based surveillance programs [conference summary]. Emerg Infect Dis [serial on the Internet]. 2006 Mar. doi:10.3201/eid1203.051335
- Van Beneden CA, Lexau C, Baughman W, et al. Aggregated antibiograms and monitoring of drug-resistant Streptococcus pneumoniae.Emerg Infect Dis. 2003;9(9):1089–95. doi: 10.3201/eid0909.020620.
- Schrag SJ, Zell ER, Schuchat A, Whitney CG. Sentinel surveillance: A reliable way to track antibiotic resistance in communities?Emerg Infect Dis. 2002;8(5):496–502. doi: 10.3201/eid0805.010268.
- EM100 Connect - CLSI M100 ED34:2024. Accessed January 3, 2025.